


Amid ‘Huge’ Geopolitical Pressures, WHO Pandemic Talks Co-Chair Hopes for December Deal/ Kerry Cullinan
I just found this. Its author does not always get everything right. But it is a reasonable facsimile of where the Treaty is at.

21/11/2024 • Kerry Cullinan
CAPE TOWN – Warning that the process of negotiating a pandemic agreement has days not months left, talks co-chair Precious Matsoso hopes that a deal will finally be clinched at the next meeting of the Intergovernmental Negotiating Body (INB) in early December.
“We don’t have six months left to finish negotiations. We only have a couple of days left, precisely because the geopolitical environment is so challenging. There is huge, huge pressure on the talks and we don’t know what the outcome will be,” said Matsoso of the negotiations by World Health Organization (WHO) member states on an internationally binding accord that aims to better prepare for, and respond, to the next pandemic. [Matsoso exaggerates here about only having days—Nass]
The cloud hanging over the talks is the distinct possibility that President-elect Donald Trump would pull the United States out of the negotiations, or even out of the WHO, after he takes office on 20 January.
The signals are hard to ignore in light of his decision to withdraw from the global health agency during his last term as president, as well as his recent nomination of vaccine skeptic Robert F Kennedy Jr, as secretary of Health and Human Services. The US withdrawal from the talks could set off a chain reaction from other conservative states that torpedoes the remaining goodwill among WHO member states, which must find a consensus on the text.
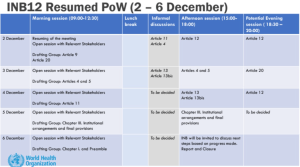
The talks resume on 2 December and run until 6 December with a crammed agenda dedicated to the most contentious issues: ‘One Health’ in the context of pandemic prevention, a mechanism for Pathogen Access and Benefit Sharing (PABS), and whether sharing of vaccines, medicines and therapeutics for use as comparative products in clinical trials should be voluntary or not.
Tit-for-tat annexes
Recalling that the negotiations started in February 2022, just a day after Russia invaded Ukraine, Matsoso said she was reflecting on 1,000 days of work, which started with a blank page.
The draft agreement has been built around five areas: prevention, equity measures, health systems, financing and governance.
The Latest Draft Pandemic Agreement (15 November at 17.14 CET) shows that much of the text has already been agreed (highlighted in green) or mostly agreed (yellow).
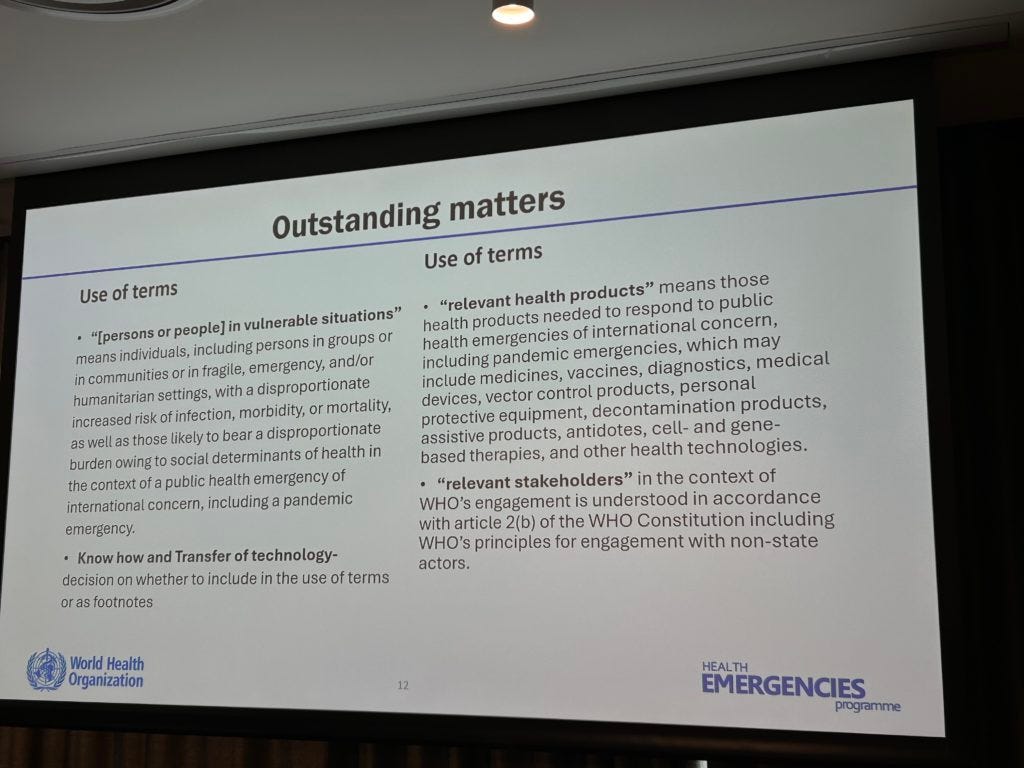
While settling some of the contested clauses is challenging, other disagreements – like whether to use the term ”people” or “persons” – appear silly.
“Some negotiators lose touch with reality,” Matsoso admitted. “Our job is to bring them back to reality.”
The two dominant negotiating blocks – represented by the Africa Group, on the one hand, and the European Union and USA on the other – are deadlocked over Articles 4 and 5 (Prevention and One Health) and Article 12 (Pathogen Access and Benefit Sharing, or PABS).
The Africa Group is reluctant to agree to an annex linked to Article 4 that lists countries’ responsibilities to prevent pandemics (including better surveillance of humans, animals and the environment for threatening pathogens) unless there is also an annex related to the operationalising of a system for PABS.
What the Africa Group wants from PABS is preferential access to any pandemic-related products that are developed from them sharing information about pathogens of concern.
The group is also concerned that a prevention annex could impose costly requirements that they are unable to finance. However, the first beneficiaries of prevention measures are individual countries’ citizens who would be protected by, for example, heightened surveillance of bats that harbour Ebola and Marburg.
“These two areas are the make-or-break articles of the negotiations. If we can reach agreement on these, we will make the deal,” Matsoso noted.
Disagreement centres on a handful of words
In some cases, a handful of words and phrases obstruct agreement.
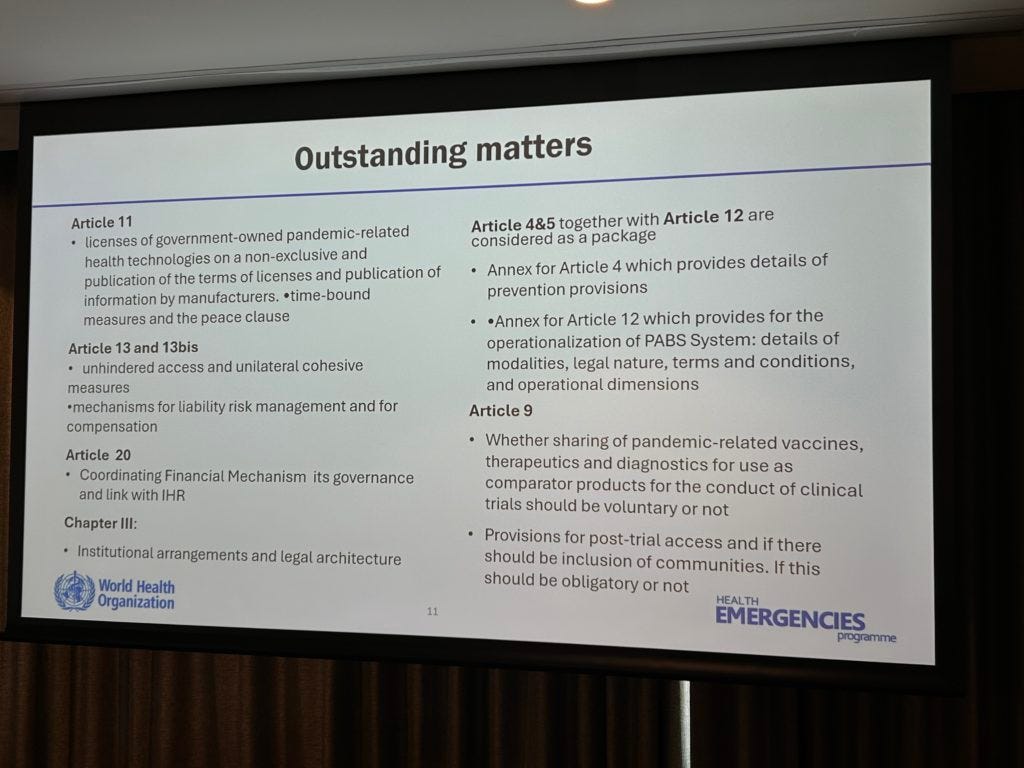
“Voluntary” is one of the sticky words. In the case of research and development (Article 9), the final outstanding issue relates to whether it is possible to compel industry to provide people who take part in clinical trials access to whatever products arise – or whether this should be voluntary. Related to this article, there is a push for trialists’ communities to also get access to these products.
This word crops up again in connection with technology transfer (Article 11) – and whether this should be mandatory or voluntary or on “mutually agreed terms”.
The other sticking point in Article 11 is whether the terms of the licences of “government-owned health technologies” related to pandemic products should be made public.
Although it may seem like a no-brainer that taxpayers should have the right to know where their money goes, pharmaceutical companies often like to keep the terms of these agreements secret.
Ten countries are pushing for the term “unhindered access” to be included in Article 13 and 13 (bis) dealing with the logistics and procurement of pandemic products. The 10 – including Russia, Iran, Syria, North Korea and Cuba – face “unilateral coercive measures” (sanctions) and want these lifted during pandemics.
“This is one of the difficult issues that the Bureau has to deal with, and we have to ensure that the pandemic agreement doesn’t become a platform for other issues,” Matsoso noted.
What’s in a word?
Some outstanding clauses can simply be resolved if negotiators agree on definitions, said Matsoso.
Agreement on “relevant stakeholders” would resolve 18 paragraphs; “know-how” would resolve eight paragraphs; “voluntary” would resolve six; “mutually agreed”, five. Deciding on “persons or people” would also resolve five.
Despite the two substantial issues and the many ratty little details, Matsoso is hopeful that negotiating parties will reach agreement at the next short meeting between 2-6 December.
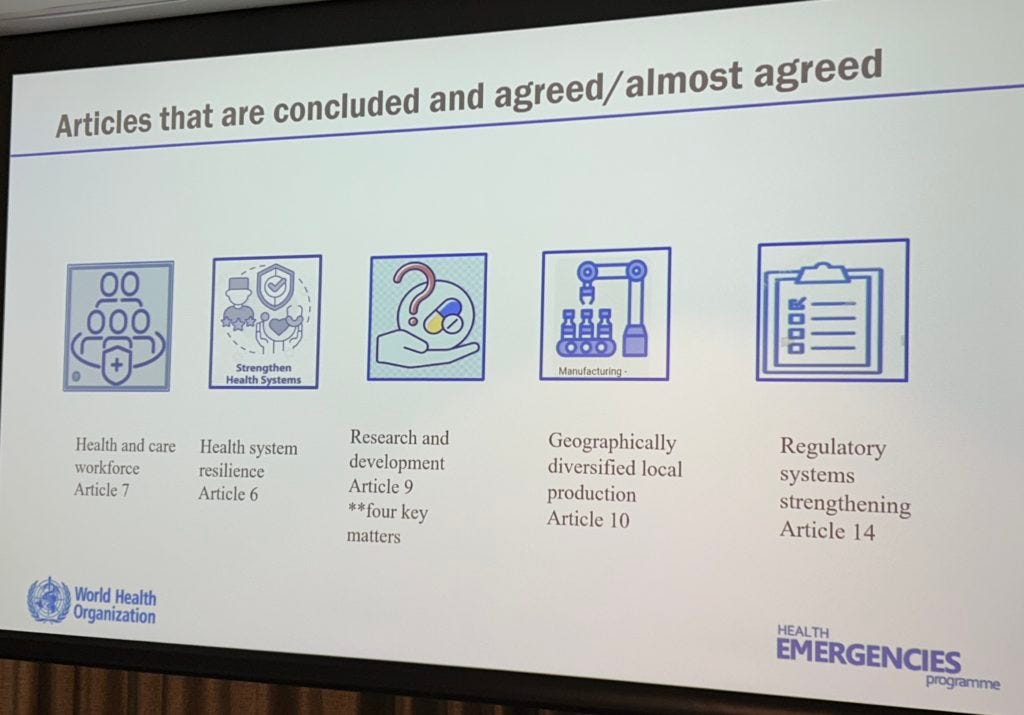
But, she notes, there is agreement on five major areas (give or take the odd phrase) – health system resilience (Article 5), health and care workforce (Article 6), R&D (Article 9), geographically diverse local production (Article 10) and regulatory systems strengthening (14).
“If we adopted this draft tomorrow, it would ensure health workers are protected, there are measures to build resilient health systems and regulatory systems are strengthened. But these provisions alone aren’t sufficient,” said Matsoso.
That last sentence is nonsense, and minor word changes are not really an issue—but the rest of this seems generally in line with my reading.—Nass
Thank You, Dr. Nass, while these paid puppets argue over words. The fact is that we don't want any of it. I hope that The Trump administration defunds the whole of The United Nations and the W.H.O. - these folks are marching forward as if 20 million people have not been injured and maimed, and the millions dead. It is absolute insanity and is not in any way shape or form a medical and health purpose line. The original charter of the United Nations in 1947 calls for "controlling the population". It is yet another agency built for the sole purpose of fleecing Nations of their Health and their Wealth. IMO. Thank You for keeping us up to date with what is happening. xoxoxo Happy Holidays.
The Ukraine conflict rages on, nary a peep from the human carnage. The UN seems to be a victim of mission creep