


Plea to African Union: Halt votes on WHO pandemic agreement and international health regulations amendments

Dear Ministers of Health in Africa,
The Pan-Africa Epidemic and Pandemic Working Group calls on the African Union to table a motion to postpone the votes for the draft World Health Organisation (WHO) Pandemic Agreement and amendments to the International Health Regulations (IHR).
The working group is a network of senior African academics from a variety of disciplines committed to advocating for sound public health policies at the national, regional and global levels.
It has come to our notice that the WHO is finalising negotiations on the draft Pandemic Agreement (formerly called the Pandemic Treaty) and amendments to the IHR. These instruments are designed to provide the WHO with new and greater powers. More specifically, they would give the WHO director general authority to personally declare a public health emergency of international concern, and thereafter to exercise unprecedented sweeping powers over all state parties to the proposed instruments.
We are particularly concerned about five issues.
1. Conflicts of interests
The WHO is significantly privately funded by corporations and individuals based in wealthy countries who directly benefit from the pharmaceutical and digital health aspects of the proposals in the two instruments. In addition, much of WHO’s programme is now determined by its largest funders — wealthy countries with strong Pharma sectors (US and Germany), and the Bill and Melinda Gates Foundation, through specified funding under which the WHO works for the purpose for which the funding was given. As such, the views of the vast majority of states have very little impact on the actual operations of the WHO, and this is a clear erosion of their national sovereignty.
2. Poor WHO Covid-19 response track record
The WHO’s track record in the Covid-19 response is poor, including:
Policies such as lockdowns that have been previously acknowledged by the WHO itself to cause significant collateral harm, and having disproportionately negative effects on low-income populations and countries in Africa;
Discouraging the use of affordable repurposed drugs and promoting new drugs under Emergency Use Authorisation (EUA);
Promoting mass and often mandatory vaccination against Covid-19 of African populations known to be very low risk due to young age and already having immunity, thereby diverting resources from malaria, tuberculosis, HIV/Aids and other urgent health problems on the continent, and violating the right to informed consent;
Inaction and lack of accountability regarding vaccine injuries and deaths;
Disruption of economies and education, entrenching future poverty and multi-generational inequality, and expanding national debt directly correlated to the debt crisis in Africa today; and
Promoting censorship in the guise of tackling “misinformation” and “disinformation”, thereby stifling civil liberties and academic freedom.
Thus, the Covid-19 response has already centralised control, and further concentrated wealth in high income countries while impoverishing low-income populations, including those in Africa. It has expanded an increasingly colonialist agenda in Africa with substantial negative economic, human rights, socio-cultural and political consequences.
The lockdown regulations were a class-based and unscientific instrument, disproportionately harmful to lower-income people and useless for crowded informal settings as in urban parts of Africa. At the same time, African governments were subjected to intense pressure to merely adhere to protocols formulated outside the continent and in total disregard of their demographic, economic and climatic contexts. This rendered them powerless on public health matters in their own jurisdictions, which was tantamount to the eroding of their health sovereignty with predictable and harmful consequences.
It is therefore evident that the WHO Pandemic Agreement and Amendments to the IHR, if signed in their current form by the requisite number of WHO member states in May/June 2024, will entrench all the measures above in international law, institutionalising the withdrawal of health sovereignty and economic sovereignty from African states.
3. Procedural injustice, democratic illegitimacy and inequitable outcomes
The adoption of any amendments to the IHR at the 77th World Health Assembly in May 2024 are being processed in an unlawful manner. Article 55(2) of the IHR sets out the procedure for amending these regulations:
The text of any proposed amendment shall be communicated to all states parties by the director general at least four months before the Health Assembly at which it is proposed for consideration.
The deadline for the WHO’s director general to circulate the package of proposed amendments to the IHR to state parties lawfully in advance of the 77th assembly was 27 January 2024, and yet the text is still being negotiated, with a version released to the public in mid-April 2024. As such, the agenda item of passing the amendments to the IHR cannot be legitimately tabled at the assembly, as tabling it without complying with the requisite four-months rule would jeopardise procedural justice, democratic legitimacy and equitable outcomes for all.
The review time is essential for each state party to assess national health, financial, legal and human rights implications, and the abrogation of this rule by the WHO disproportionately discriminates against lower-income countries with fewer resources to rapidly assess such consequences. The Pandemic Agreement, also still under negotiation, was intended to be delivered by 29 March 2024, for a similar intent of providing time for reflection prior to commitment to vote.
4. The inadequacy of a one-size-fits-all approach
Flexibility and careful public health planning are crucial given the highly diverse economic, demographic, cultural and environmental factors that render the current WHO one-size-fits-all approach grossly inadequate. In particular, African societies continue to heave under the burden of preventable diseases such as infections including malaria, HIV/Aids and tuberculosis, along with a high prevalence of malnutrition which fuels high death rates from the above diseases. As such, placing a financial burden on these societies through non-priority globalised pandemic preparedness initiatives is an instance of misplaced priorities and intrinsically inequitable.
Furthermore, the WHO is laying inordinate emphasis on pandemic preparedness in terms of the framework it used at the height of Covid-19. As such, it does not address the manner in which the most vulnerable in societies were dragged deeper into poverty from this centralised approach with an emphasis on costly pharmaceutical interventions and discouragement of the use of affordable repurposed therapeutics while ignoring building of resilience through nutrition and sanitation. It is noteworthy that a tiny minority became markedly wealthier from the centralised approach, thus entrenching global inequity.
5. Exaggerated urgency for the Pandemic Agreement and amendments to the IHR
The WHO has consistently asserted that urgency in enhancing the world’s capacity to address pandemics through instruments such as an amended IHR and the draft Pandemic Agreement is justified by a rising risk and burden of infectious disease outbreaks from pathogens transferred from animals to human beings. However, a report from the University of Leeds released in early 2024 has demonstrated this to be a markedly exaggerated claim. According to that report, the evidence bases on which the WHO and partner agencies including the World Bank and G20 have relied actually demonstrate that the risk of naturally-derived outbreaks is not currently increasing, and the overall burden is probably declining. This suggests that current mechanisms are indeed working relatively effectively, and changes must be viewed carefully, without undue urgency.
Our Petition
In view of the foregoing considerations, we call on the African Union to table a motion at the 77th World Health Assembly in May 2024 to halt the process of enacting the draft Pandemic Agreement and Amendments to the International Health Regulations until the following measures have been put in place:
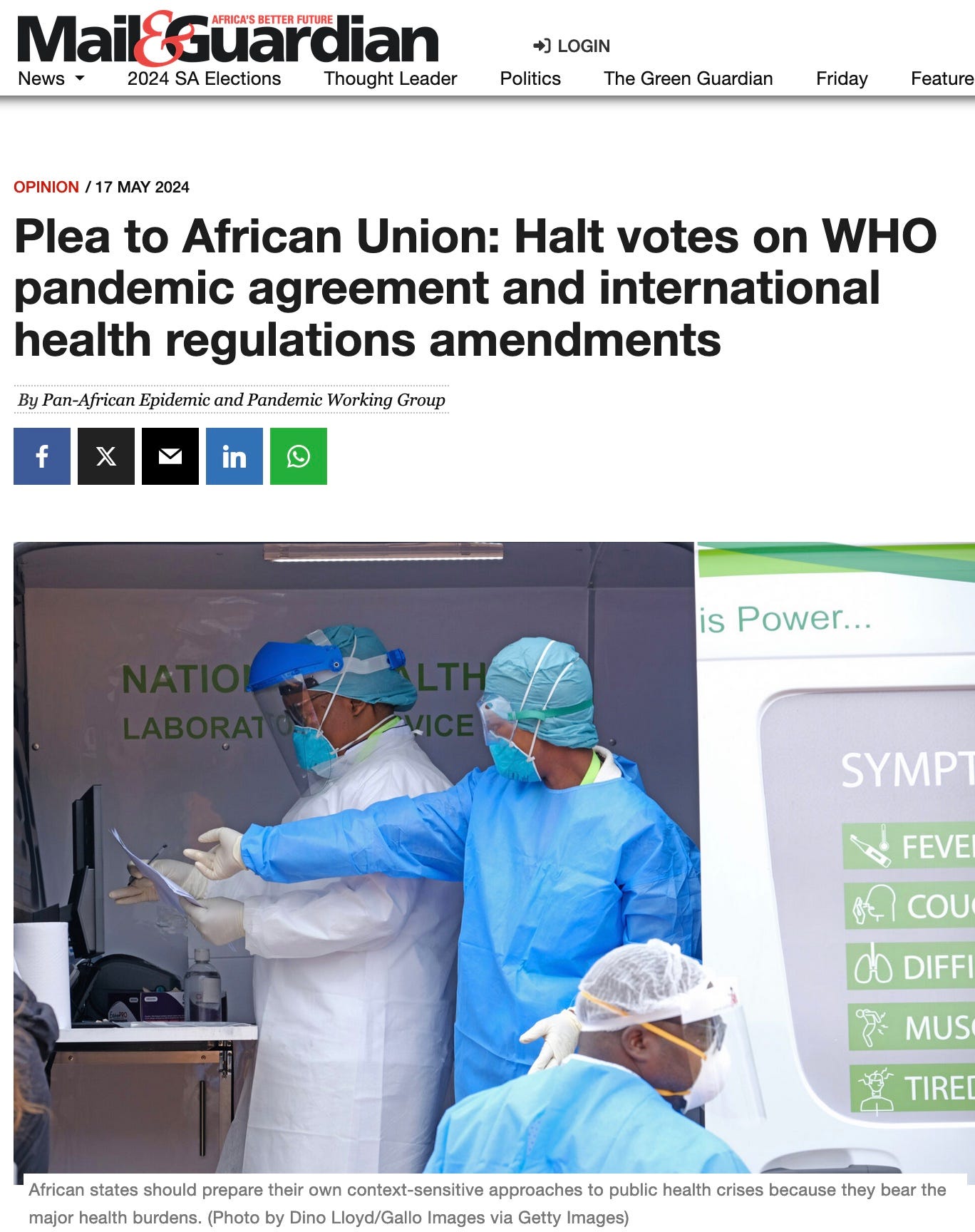
Affirm and respect the right of African states to freely prepare their own context-sensitive approaches to public health crises.
Facilitate a transparent and accountable review of the role of Western-based international governmental and non-governmental health entities in the WHO’s operations and policies. Such a review must ensure the full participation of African countries, because they are the bearers of the major health burdens.
Facilitate a re-orientation of international public health to a population-based and disease burden-based approach in line with the WHO’s own stated commitment to primary health care entailing the robust participation of communities.
Yours sincerely
Dr Carlos Cardoso, director of the Centro de Estudos Sociais Amilcar Cabral (Amilcar Cabral Centre for Social Studies), Bissau. carlos.cardoso28@gmail.com
Dr Fernandes Wanda, coordinator of the Centre for Social and Economic Research, Faculty of Economics, Universidade Agostinho Neto, Angola. fernawan@hotmail.com
Professor Francis E Onyango, associate professor of paediatrics and child health, Uzima University, Kisumu, Kenya. onyangof@yahoo.com
Professor Olutayo C Adesina, professor of history, University of Ibadan, Nigeria. olutayo27@gmail.com
Professor Pedrito Cambrao, assistant professor and the scientific deputy at the Faculty of Social Sciences and Humanities, Universidade Zambeze (UniZambeze), Mozambique. Prof.Pedrito@hotmail.com
Professor Reginald MJ Oduor, associate professor of philosophy, University of Nairobi, Kenya. rmjoduor@gmail.com
Dr Samuel Adu-Gyamfi, senior lecturer and head of department of History and Politics, Kwame Nkrumah University of Science and Technology, Ghana. mcgyamfi@yahoo.com
Professor Wellington Oyibo, College of Medicine, University of Lagos, Nigeria. wellao@yahoo.com
Professor Divine Fuh, associate professor of social anthropology and director of the Institute for Humanities in Africa, University of Cape Town, South Africa. divine.fuh@uct.ac.za
My friends, I need your help to share THE FIRST Narrative Feature Film EXPLOITING THE CORRUPTION OF COVID by Michael Angel Loayza Jr. (a Conscious Filmmaker)
https://youtu.be/1KjgGgaJBaE?si=eXTF9vGpcnlc7J2r
We must all peacefully work together to exploit the corrupt institutions and to no longer be a slave to their toxic, greed-riddled agenda.
Please, reach out, Like, Subscribe on YouTube and Instagram
Totally intelligent and lucid response to this underhanded and devious Pandemic Treaty. It was not presented on time and the presenter is a con artist from the get go with no medical or health credentials. His resume as TERRORIST...THIEF...MURDERER would not recommend anything he presented to be accepted, if the IHR were comprised of honorable and ethical humans..