

Today's ACIP (CDC advisory committee) meeting: quick summary. COVID vax to be discussed tomorrow.
Today's ACIP (CDC advisory committee) meeting: quick summary. COVID vax to be discussed tomorrow.
It ended with yet another paean to the chickenpox vaccine, as if to say that despite the COVID, Dengue and Chikungunya vaccines, they did approve something useful, once upon a time

Six vaccines and a monoclonal were discussed today. Here is where you can watch the meeting and read my commentary, and also see comments made by others who are watching. 8 am-2 pm tomorrow will cap off this meeting.
There are 2 existing Meningococcal vaccines currently, for Neisseria meningitidis serotypes ACWY and B. N. meningitidis causes very serious meningitis and sepsis—but cases are VERY RARE. One per million Americans per year. About 300 cases per year. But many millions of people carry N. meningitidis bacteria in their noses.
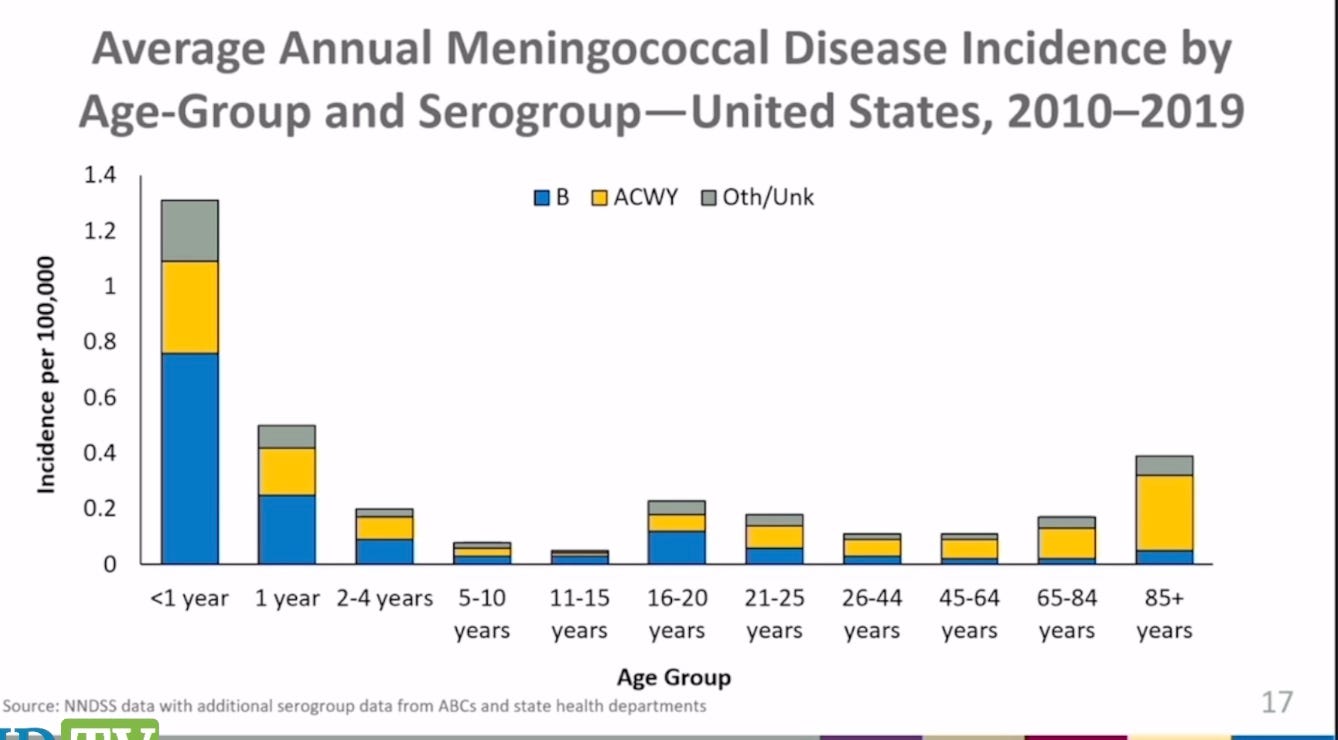
The chart below, used at the ACIP meeting, peculiarly misleads on overall incidence, by using 4 bars for the first 10 years but only one bar for 20 year intervals in older adults. According to CDC, “Rates of meningococcal disease have declined in the United States since the 1990s and remain low. In 2019, there were about 375 total cases of meningococcal disease reported (incidence rate of 0.11 cases per 100,000 persons).”
So the question is, do the vaccines prevent disease? The number of cases had been rapidly decreasing for many years (reason obscure) before there was general use of the vaccines. The vaccines don’t last long, if they do work. Maybe 4 years. What about side effects? That is unclear.
A data-free decision was made to give the Men A vaccine to kids aged 12 and 16, allegedly cause they were at higher risk in high school and in college dorms. Higher, yes, just a tad, but you have to vaccinate millions of kids to prevent one case. Never made sense. Wears off before college is over.
Now the plan is to put together a Men A and a Men B vaccine in one shot. Both Pfizer and GSK are doing it, why not? It would add the B vaccine to the childhood schedule, takes almost no work since they already have the components. What a moneymaker—taking two vaccines that likely do more harm than good, just mix them together. Schizer currently charges (retail) $148 for the ACWY vaccine and $180 for the B vaccine, per dose.
So Pfizer threw a few antibody tests together and called it good, having learned from COVID you don’t need evidence of safety or efficacy any more.
Serious Adverse Events in Pfizer’s trial: 2 suicide attempts, 1 case of POTS developed, 1 "spinal cord injury"--might that be transverse myelitis? Sounds like these 4 could be vaccine injuries. 2 more severe depression . 1763 total subjects 10-26 years old. 70% Americans, the rest from EU. Dr. Lehrer says he is glad the vaccine "works" but he notes that there are only 1 case in a million--but there are serious adverse reactions noted in 1 in 2-300.
BTW, if you have a headache and fever and stiff neck—or any 2 out of three—go to the ER because this form of meningitis is a bacterial illness and an antibiotic received quickly is life-saving.
The ACIP actually wanted more info, so Pfizer promised to pull some together and come back.
POLIO. We use the injected vaccine with 3 serotypes for this viral illness. The CDC briefer actually told some truths. We gave up the stronger oral vaccine in 1999 because it was causing polio in several cases a year, and we switched to the killed, injected vaccine. The problem is that it barely works. It does not prevent transmission. WAIT WHAT?
Are we back to COVID-like vaccines? Is this another Potemkin village vaccine?
One polio case in New York occurred, as it was bound to do at some point, because CDC, while coy, new all along that some people shed virulent polio virus forever—as the vaccine strains have long proven their ability to revert to virulence. That is why we stopped using them in 1999. This was the first home-grown polio case in 2 decades. So CDC is revisiting how we manage polio.
It is a good question, because we cannot get rid of polio because many people still receive the live, oral vaccine and so some people excrete virulent polio virus. Most cases of polio in the world come from polio viruses that developed from live vaccines. ACIP will in future vote on keeping current recommendations in place.
RSV. Respiratory Syncytial Virus. Wondering why you just started hearing about it this year? That is because the industry developed 3 new RSV products: a vaccine for pregnant people (just kidding!) a monoclonal antibody for newborns and a vaccine for the elderly. THAT is why you have been hearing about it.
Finally, however, briefers admitted that we don’t actually know how much of a problem RSV is, especially in the elderly. And it could wind up costing a million bucks per year of elderly life saved, if it is not a big problem. And the GSK version contains a novel adjuvant, ASO1, which can overstimulate the immune system, which is why it is only used for the elderly or immunocompromised. Pfizer has developed a different RSV vax for elders.
However, it looks like the pregnancy vaccine and the newborn monoclonal will definitely be a go, as these people have never seen a vaccine they didn’t like. And there was no useful safety data nor efficacy data presented. But there was a whole lotta modelling going on.
CHIKUNGUNYA. As someone pointed out today, the name may change, as it could stigmatize chickens, chicks and gun owners. Why are we talking about a vaccine for this condition? Hardly any Americans have ever had it, almost all travelers, and it is not endemic anywhere in our country. You get the virus from mosquito bites. Bug repellent protects you.
Furthermore, how is it that FDA gave this vaccine a “Priority Review”—a promise to speed up its evaluation and make a decision within six months?
There are criteria for a priority review, and this vax does not meet them. From the FDA website:
A Priority Review designation will direct overall attention and resources to the evaluation of applications for drugs that, if approved, would be significant improvements in the safety or effectiveness of the treatment, diagnosis, or prevention of serious conditions when compared to standard applications.
Significant improvement may be demonstrated by the following examples:
evidence of increased effectiveness in treatment, prevention, or diagnosis of condition;
elimination or substantial reduction of a treatment-limiting drug reaction;
documented enhancement of patient compliance that is expected to lead to an improvement in serious outcomes; or
evidence of safety and effectiveness in a new subpopulation.
CDC expects a license in 6 months and a rollout in 12. The reason this disease needs to be conquered is that it causes a lot of chronic joint pains. But we don’t know how much, since the 27 studies CDC evaluated were all over the map. Never mind—it causes a problem and CDC is here to solve it.
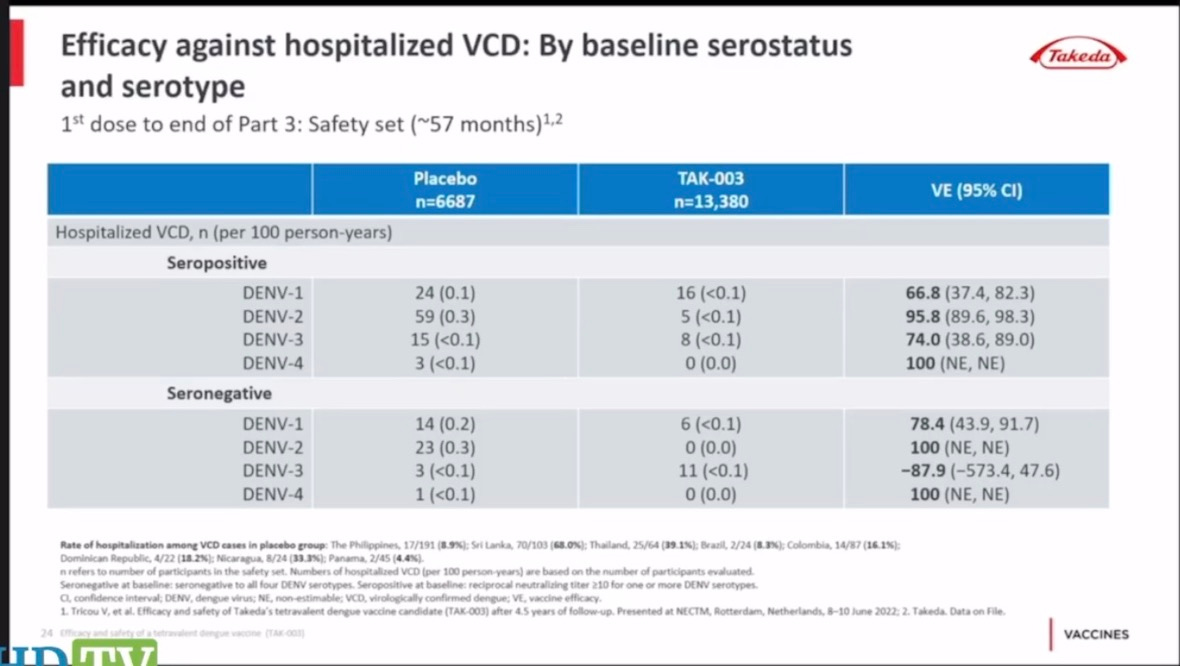
DENGUE. Another mosquito-borne viral disease. There is already a licensed vaccine on the market, but now another one approaches. The licensed one, from Sanofi, killed a lot of kids in the Philippines and Sanofi staff and government official were charged with murder. So we licensed it here, but required that kids prove they already had one of the four strains so they don’t die too.
Anyone else find it odd that being seropositivie offered no protection, but the vaccine did?

This new vaccine shows no evidence of benefit for the DEN4 serotype, and seems to enhance the DEN3 disease—just like COVID vaccines make you more susceptible to COVID after a few months go by.
I don’t know about you, but to me it seems there is too much fat on the vaccine bone. The industry ran out of targets at home, so now they are using a shotgun to find exotic new diseases to worry about. Obama said vaccines must be “free” if you have insurance, and the industry saluted, and here we are. Will an elephantiasis vaccine be next on the childhood schedule?
Sounds like the c19 vaccine taught big pharma that they can get away with murder.
Dr. Nass, with all these extra jabs coming down the pike, many states will add them to the childhood vaccine requirements to go to school. Places like NY have completely eliminated religious exemptions. With your work at CHD, is there any talk of suing these states so there can again be religious exemptions? Homeschooling is not always an option for parents. Thank you for all you are doing to keep us informed.