


An analysis of Articles 1-9 in the adopted vs proposed IHR, as requested by many
Analysis of later articles will be coming. The skinny on why this was a big win.


Below, I will be comparing the WHO's initially proposed International Health Regulations (IHR) amendments of 6 February 2023 with what actually got passed (adopted) on June 1, 2024--because there has been an extraordinary amount of confusion about this in the media. Please remember that I am a doctor, not a lawyer and these are my impressions. I will only comment on things I think are of particular relevance.
Here is something else there is confusion about: the adopted changes will not go into effect for 12 months for most countries and 24 months for others. So the version of the IHR that is in force currently is the (2005) version, which went into force in 2007. The bolding and crossed out words are the changes to this 2005 version.
Above I screenshot both document titles so you can see which 2 documents I am comparing. All 3 versions of the IHR are hyperlinked in the above 2 paragraphs so you can evaluate them for yourself. I also include some screenshots in this compilation.
Below is the key for understanding the meaning of the bold language and struck through language in the 6 February 2023 proposed amendments.
Article 1 Definitions
Article 1 as proposed crossed out "non-binding" for both temporary and standing recommendations. This meant that all "recommendations" were to become binding "advice." In other words, they would no longer fit the meaning of recommendations or advice, and instead they would become orders. This was tricky language some lawyer for the WHO came up with, but it was almost immediately exposed. People did not like it.
In the adopted version, "non-binding" is no longer crossed out. This means that all recommendations and advice have returned to their clear meaning (recommendations only) and there is no requirement that nations comply with the "advice." This is extremely important because it removed the teeth from nearly every article in the rest of the document.

Article 2 Purpose and Scope
Article 2 as adopted got rid of the claim that the purpose of the IHR included "health systems readiness and resilience"--which is good, because the proposed terminology was very loose, and a lot of requirements for health systems could be snuck in later as being necessary for readiness or resilience.
The current (2005) version of the IHR noted that public health responses should be a) "commensurate with and restricted to public health risk" and b) "avoid unnecessary interference with international traffic and trade."
The proposed version expanded possible responses to a) "all risks with a potential to impact public health"-- in other words, anything that might affect health, such as climate change, firearms, sugary drinks, or many other things.
The proposed version of b) was interesting. The meaning of the sentence was changed in the proposed version to avoid unnecessary interference with (language added:) livelihoods, human rights, and equitable access to health products and information. In other words, while such language did not fit well in a section on Scope and Purpose, it was placed there in order to sneak in the word "unnecessary." What the sentence then indicated is that it would be okay, when necessary, to interfere with livelihoods, human rights, and equitable access to health products and information. This was consistent with the crossing out of human rights in proposed Article 3, and the WHO’s desire to restrict information, and therefore I believe this very concerning sentence was intentionally designed to shaft human rights, equitable access to medications and information and bless interference with livelihoods (i.e., lockdowns, etc.)
All the worrying changes in the proposed IHR Article 2 that I just described were not included in the amendments that were adopted.
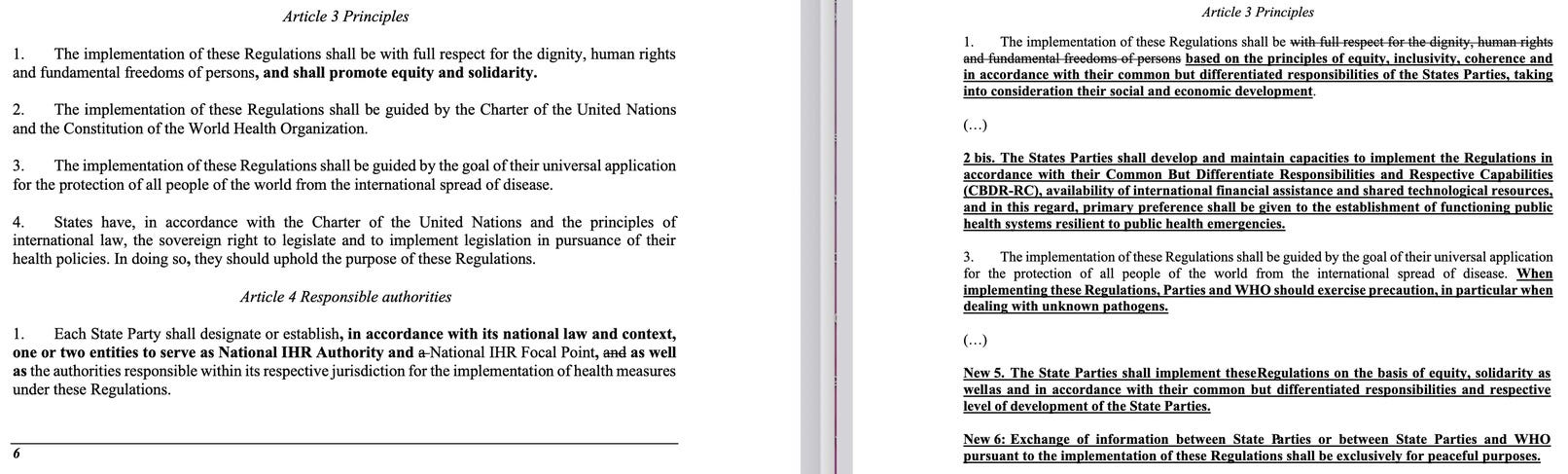
Article 3 Principles
The proposed Article 3, paragraph 1 attempted to fool readers by removing the existing IHR language, which guaranteed that implementation of the IHR must respect "dignity, human rights and fundamental freedoms of persons." These are rights that are specifically laid out in UN treaties and other documents. The proposal replaced this with language that did not have legal meaning and was ambiguous besides, while intended to convey an aura of "equity." The replacement language was: "based on the principles of equity, inclusivity, coherence."
The adopted Article 3 paragraph 1 amendment retained all the original language that guaranteed rights, while adding the words equity and solidarity: "The implementation of these Regulations shall be with full respect for the dignity, human rights and fundamental freedoms of persons, and shall promote equity and solidarity." No rights were lost, and equity and solidarity were added. Of interest, neither equity nor solidarity are defined in the extensive list of definitions in Article 1.
Paragraph 2 simply states an old fact: the IHR implementation should conform with the UN Charter and WHO Constitution. Just like US law must conform with the Constitution. I am not sure why people took issue with this.
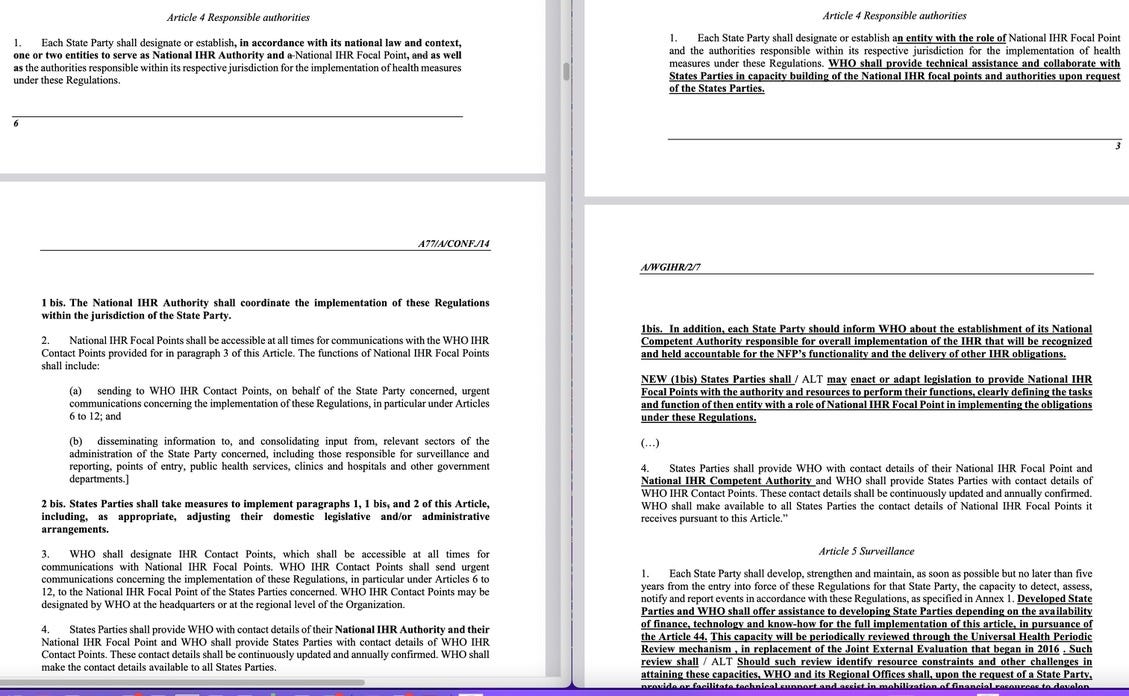
Article 4 Responsible Authorities
There already exists a "National IHR Focal Point" in every nation whose role is to notify the WHO of possible outbreaks, etc. This is an old requirement.
Article 4 creates a second entity, the "National IHR Authority" in each nation, but allows nations to have one entity serving both roles. The role of the IHR Authority is to implement the IHR regulations. Note that in the proposed version, this entity would be "held accountable" for delivering IHR "obligations"--in other words, nations would be forced to comply with their "obligations." All this accountability language was been removed from the adopted version.
Paragraph 2 is about getting information to the WHO in a speedy fashion, through the Focal Points and Contact Points. Since one of the main reasons to amend the IHR, according to the US, was to be sure that pandemics will not be hidden by national governments, it makes sense that the state parties demand details about how the information about possible outbreaks will be passed on and who will be responsible for doing so.
In paragraph 3 of the proposed IHR, nations were to be asked or required to pass legislation to give power and funding to the Focal Points. This language, reproduced below, is gone in the adopted IHR.
NEW (1bis) States Parties shall / ALT may enact or adapt legislation to provide National IHR Focal Points with the authority and resources to perform their functions, clearly defining the tasks and function of then entity with a role of National IHR Focal Point in implementing the obligations under these Regulations.
Article 5 Surveillance
This adopted article newly establishes the norm that nations will be expected to meet core capacities in their public health response within 5 years, or longer if an extension is granted. WHO is to assist developing nations meet this requirement, but it is not stated what WHO must do. Open-ended, more extensive requirements in the proposed version were not included in the adopted version. One African nation (Uganda?) noted in its discussion after the new IHR was adopted that it has little outbreaks all the time and it would be onerous and unrealistic to require early reporting of all of them. This statement portends that African nations may issue reservations or rejection of the surveillance and notification provisions of the adopted IHR. They have 10 months (or for a few nations, 18 months) to do so.
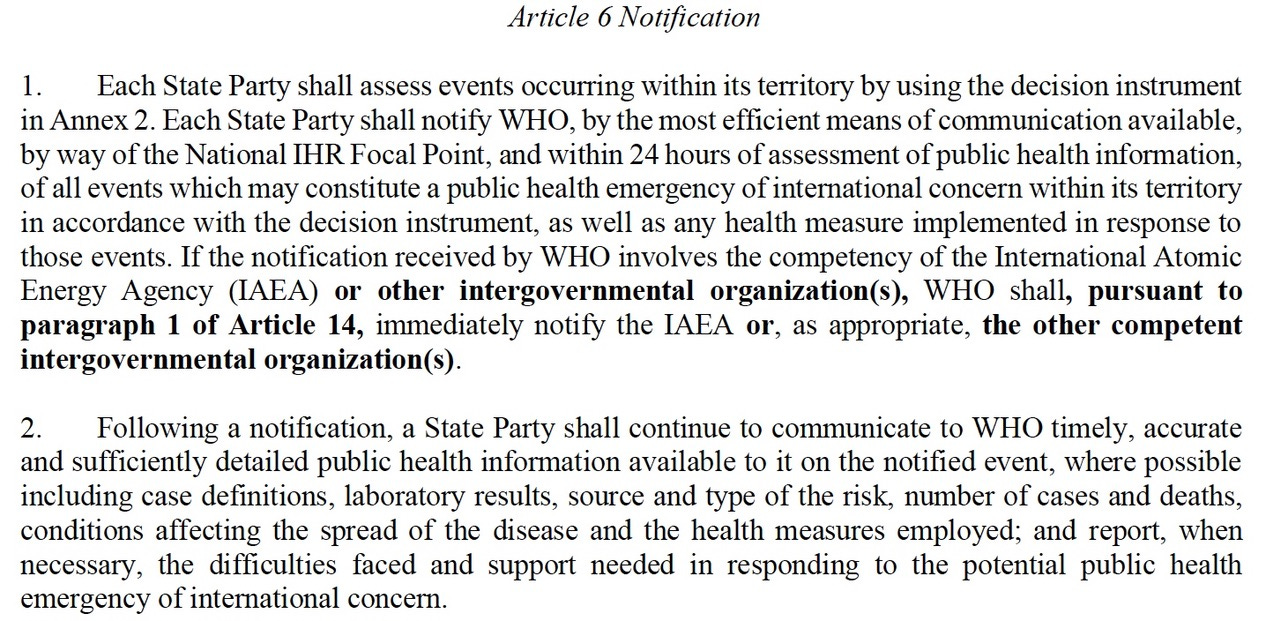
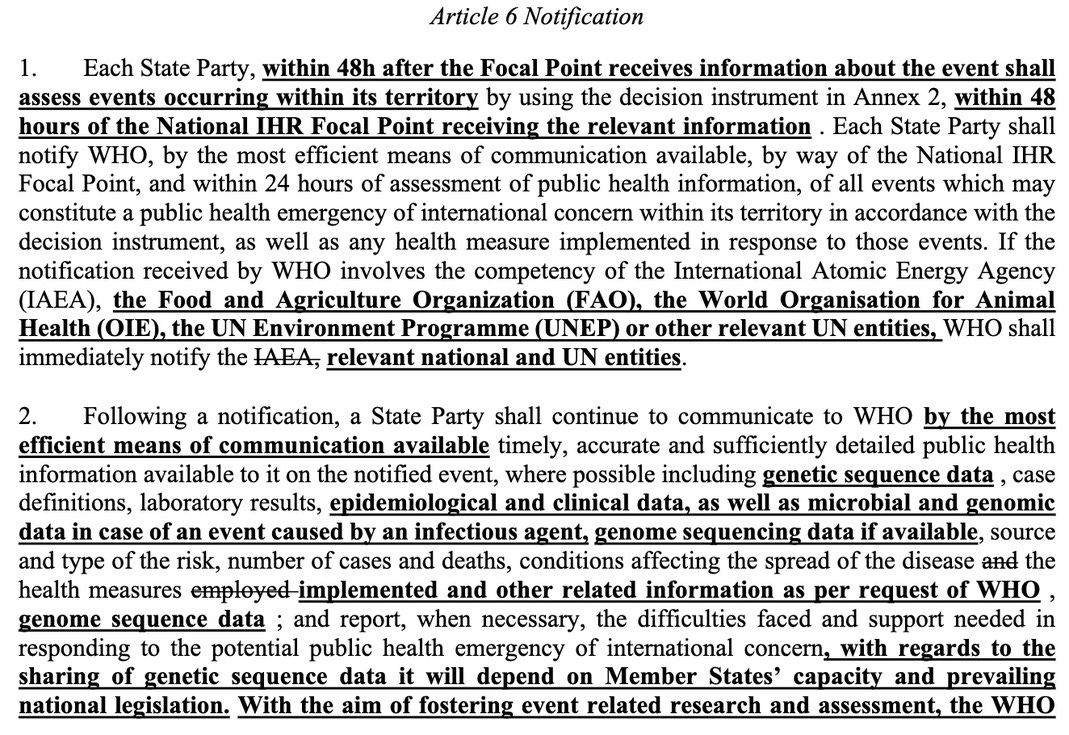
Article 6 Notification
The proposed Article 6 wanted very specific genetic sequencing data, specimens, and detailed epidemiological information from nations with an outbreak. The WHO would then share this information with all Parties. This was not adopted.
The proposed version then stated (disingenuously) " WHO shall not transfer the public health information received...[to entities] engaging directly or indirectly with conflict and violence elements." I found this proposal horrifying: WHO planned to share pandemic pathogens with anyone who wanted them, with the exception of those "engaging... with conflict or violence elements"? Why did WHO plan to proliferate microorganisms that could cause pandemics? The WHO's use of this language seemed to me to be an attempt to obtain tacit agreement from nation states for widespread proliferation of what the WHO termed “potential pandemic pathogens.”
The adopted Article 6 fails to say anything about the WHO transferring materials. It omits the terms "genetic sequence data" and while it requires information, it is much less specific about what information nations must provide.
Article 7 Information-sharing during unexpected or unusual public health events
The proposed language demanded that nations supply microbial samples and genetic sequence data to WHO. The adopted language simply says nations will supply all relevant public health information. I was struck by how aggressively the WHO demanded genetic sequence data in many versions of the documents (and there were also demands that nations build sequencing labs, potentially to sequence the genes of citizens in 196 countries—which was not adopted) and I was pleased that such language was removed everywhere from the IHR.
Article 8 Consultation
Not much of significance changed
Article 9 Other Reports
The proposed article removed the requirement that the WHO would have to consult with the nation in whose territory an outbreak was occurring before taking action. This was not removed in the adopted version. WHO would continue to be required to consult with a nation before taking actions regarding that nation.
This wording was proposed:
(New wording) "In the recommendations made to the States Parties regarding the collection, processing and dissemination of health information, WHO could advise the following: (a) To follow the WHO guidelines on criteria and analogous modes of processing and treating health information."
Remember that in the proposed version, 'advise' could mean "order' (if the term 'non-binding' had been eliminated as proposed, which did not make it to the adopted version). This would have given WHO wide berth to demand whatever information it desired and would have allowed WHO to do whatever it wanted with the information. It was not adopted.
Thanks for doing this Dr Nass. It did clear things up a bit for me. Ultimately, we still need to completely get rid of the "WHO", but at least this is something. Personally, I didn't plan on complying with anything anyway, even if the whole shebang would have been adopted with all of the tyranny included as they originally wanted. I think we forget that we the people still have incredible amounts of power. If we can't be governed... we won't be. If people just refuse to comply with insanity government and tyrants typically give up. I think it was James Corbett who said something like, "How are they going to enforce all of this in every country on the planet? Send in armed blue helmets? They don't have enough personnel to do that anyway." I always refer back to LOCAL LOCAL LOCAL. We need to make sure that our states, counties, districts, etc have sane people representing us who have the courage to say, "um... we see your insane "regulations", but we aren't going to enforce that insanity here." We can make the "WHO" and any of these other monstrous groups obsolete if we just say, I will NOT comply.
"the adopted changes will not go into effect for 12 months for most countries and 24 months for others"
Why acknowledge any effect, when they have no effect at all in the U.S., because they violate the Constitution and are therefore void ab initio, dead on arrival?