


I wrote a really important article published by Brownstone yesterday. Today my new organizations' website stopped working properly: DoorToFreedom.org
We were making great progress with it!

So, maybe it was just a wordpress glitch. Could be. It was nearly finished. The videos do not work and we cannot work on the back end right now. Buttons are missing. But we have a great team and I am hopeful it will be back up and running perfectly soon.
Here is my Brownstone article. It is long (5,000 words) and deep and wide and provides historical perspective on biowarfare and the pandemic and the WHO Treaty.
I am seeking comments about the content because I think it contains crucial information that people need to have and I want to improve the piece; in fact, I am re-editing it right now. Appreciate all your assistance.
https://brownstone.org/articles/who-amendments-increase-man-made-pandemics/

The WHO’s Proposed Amendments Will Increase Man-Made Pandemics
Meryl Nass August 17, 2023
This report is designed to help readers think about some big topics: how to really prevent pandemics and biological warfare, how to assess proposals by the WHO and its members for preventing and responding to pandemics, and whether we can rely on our health officials to navigate these areas in ways that make sense and will help their populations. We start with a history of biological arms control and rapidly move to the COVID pandemic, eventually arriving at plans to protect the future.
Weapons of Mass Destruction: Chem/Bio
Traditionally, the Weapons of Mass Destruction (WMD) have been labelled Chemical, Biological, Radiologic, and Nuclear (CBRN).
The people of the world don’t want them used on us—for they are cheap ways to kill and maim large numbers of people quickly. And so international treaties were created to try to prevent their development (only in the later treaties) and use (in all the biological arms control treaties). First was the Geneva Protocol of 1925, following the use of poison gases and limited biological weapons in World War I, banning the use of biological and chemical weapons in war. The US and many nations signed it, but it took 50 years for the US to ratify it, and during those 50 years the US asserted it was not bound by the treaty.
The US used both biological and chemical weapons during those 50 years. The US almost certainly used biological weapons in the Korean War (see this, this, this and this) and perhaps used both in Vietnam, which experienced an odd outbreak of plague during the war. The use of napalm, white phosphorus, agent orange (with its dioxin excipient causing massive numbers of birth defects and other tragedies) and probably other chemical weapons like BZ (a hallucinogen/incapacitant) led to much pushback, especially since we had signed the Geneva Protocol and we were supposed to be a civilized nation.
In 1968 and 1969, two important books were published that had a great influence on the American psyche regarding our massive stockpiling and use of these agents. The first book, written by a young Seymour Hersh about the US chemical and biological warfare program, was titled Chemical and Biological Warfare; America’s Hidden Arsenal. In 1969 Congressman Richard D. McCarthy, a former newspaperman from Buffalo, NY wrote the book The Ultimate Folly: War by Pestilence, Asphyxiation and Defoliation about the US production and use of chemical and biological weapons. Prof. Matthew Meselson’s review of the book noted,
Our operation, “Flying Ranch Hand,” has sprayed anti-plant chemicals over an area almost the size of the state of Massachusetts, over 10 per cent of its cropland. “Ranch Hand” no longer has much to do with the official justification of preventing ambush. Rather, it has become a kind of environmental warfare, devastating vast tracts of forest in order to facilitate our aerial reconnaissance. Our use of “super tear gas” (it is also a powerful lung irritant) has escalated from the originally announced purpose of saving lives in “riot control-like situations” to the full-scale combat use of gas artillery shells, gas rockets and gas bombs to enhance the killing power of conventional high explosive and flame weapons. Fourteen million pounds have been used thus far, enough to cover all of Vietnam with a field effective concentration. Many nations, including some of our own allies have expressed the opinion that this kind of gas warfare violates the Geneva Protocol, a view shared by McCarthy.
A Biological Weapons Convention
Amid great pushback over US conduct in Vietnam, and seeking to burnish his presidency, President Nixon announced to the world in November 1969 that the US was going to end its biowarfare program (but not the chemical program). Following pointed reminders that Nixon had not eschewed the use of toxins, in February 1970 Nixon announced we would also get rid of our toxin weapons also, which included snake, snail, frog, fish, bacterial, and fungal toxins that could be used for assassinations and other purposes.
It has been claimed that these declarations resulted from careful calculations that the US was far ahead technically of most other nations in its chemical and nuclear weapons. But biological weapons were considered the “poor man’s atomic bomb” and required much less sophistication to produce. Therefore, the US was not far ahead in the biological weapons arena. By banning this class of weapon, the US would gain strategically.
Nixon told the world that the US would initiate an international treaty to prevent the use of these weapons ever again. And we did so: the 1972 Convention on the Prohibition of the Development, Production and Stockpiling of Bacteriological (Biological) and Toxin Weapons and on their Destruction, or Biological Weapons Convention (BWC) for short, which entered into force in 1975.
But in 1973 genetic engineering (recombinant DNA) was discovered by Americans Herbert Boyer and Stanley Cohen, which changed the biological warfare calculus. Now the US had regained a technological advantage for this type of endeavor.
The Biological Weapons Convention established conferences to be held every 5 years to strengthen the treaty. The expectation was that these would add a method to call for ‘challenge inspections’ to prevent nations from cheating and would add sanctions (punishments) if nations failed to comply with the treaty. However, since 1991 the US has consistently blocked the addition of protocols that would have an impact on cheating. By now, everyone accepts that cheating occurs and is likely widespread.
A leak in an anthrax production facility in Sverdlovsk, USSR in 1979 caused the deaths of about 60 people. While the USSR tried a sloppy cover-up, blaming contaminated black market meat, this was a clear BWC violation to all those knowledgeable about anthrax.
US experiments with anthrax production during the Clinton administration, detailed by Judith Miller et al. in the 2001 book Germs, were also thought by experts to have transgressed the BWC.
It has taken over 40 years, but in 2022 all declared stocks of chemical weapons had been destroyed by the USA, by Russia, and the other 193 member nation signatories. The chemical weapons convention does include provisions for surprise inspections and sanctions.
Pandemics and Biological Warfare Receive Funding from Same Stream
It is now 2023, and during the 48 years the Biological Weapons Convention has been in force the wall it was supposed to build against the development, production, and use of biological weapons has been steadily eroded. Meanwhile, especially since the 2001 anthrax letters, nations (with the US at the forefront) have been building up their “biodefense” and “pandemic preparedness” capacities.
Under the guise of preparing their defenses against biowarfare and pandemics, nations have conducted “dual-use” (both offensive and defensive) research and development, which has led to the creation of more deadly and more transmissible microorganisms. And employing new verbiage to shield this effort from scrutiny, biological warfare research was renamed as “gain-of-function” research.
Gain-of-function is a euphemism for biological warfare research aka germ warfare research. It is so risky that funding it was banned by the US government (but only for SARS coronaviruses and avian flu viruses) in 2014 after a public outcry from hundreds of scientists. Then in 2017 Drs. Tony Fauci and Francis Collins lifted the moratorium, with no real safeguards in place. Fauci and Collins even had the temerity to publish their opinion that the risk from this gain-of-function research was ‘worth it.’
What does gain-of-function actually mean? It means that scientists are able to use a variety of techniques to turn ordinary or pathogenic viruses and bacteria into biological weapons. The research is justified by the claim that scientists can get out ahead of nature and predict what might be a future pandemic threat, or what another nation might use as a bioweapon. The functions gained by the viruses or other microorganisms to turn them into biological warfare agents consist of two categories: enhanced transmission or enhanced pathogenicity (illness severity).
1) improved transmissibility may result from:
a) needing fewer viral or bacterial copies to cause infection,
b) causing the generation of higher viral or bacterial titers,
c) a new mode of spread, such as adding airborne transmission to a virus that previously only spread through bodily fluids,
d) expanded range of susceptible organs (aka tissue tropism); for example, not only respiratory secretions but also urine or stool might transmit the virus, which was found in SARS-CoV-2,
e) expanded host range; for example, instead of infecting bats, the virus is passaged through humanized mice and thus acclimated to the human ACE-2 receptor, which was found in SARS-CoV-2,
f) improved cellular entry; for example, by adding a furin cleavage site, which was found in SARS-CoV-2,
2) increased pathogenicity, so instead of causing a milder illness, the pathogen would be made to cause severe illness or death, using various methods. SARS-CoV-2 had unusual homologies (identical short segments) to human tissues and the HIV virus, which may have caused or contributed to the late autoimmune stage of illness, impaired immune response and ‘long COVID.’
Funding for (Natural) Pandemics, Including Yearly Influenza, was Lumped Together with Biological Defense Funding
Perhaps the comingling of funding was designed to make it harder for Congress and the public to understand what was being funded, and how much taxpayer funding was going to gain-of-function work, which might lead them to question why it was being done at all, given its prohibition in the Biological Weapons Convention, and additional questions about its value. Former CDC Director Robert Redfield, a physician and virologist, told Congress in March of 2023 that gain-of-function research had not resulted in a single beneficial drug, vaccine, or therapeutic to his knowledge.
Nonprofits and universities like EcoHealth Alliance and its affiliated University of California, Davis veterinary school were used as intermediaries to obscure the fact that US taxpayers were supporting scientists in dozens of foreign countries, including China, for research that included gain-of-function work on coronaviruses.
Perhaps to keep the lucrative funding going, fears about pandemics have been deliberately amplified over the past several decades. The federal government has been spending huge sums on pandemic preparedness over the past 20 years, routing it through many federal and state agencies. President Biden’s proposed 2024 budget requested “$20 billion in mandatory funding across DHHS for pandemic preparedness” while the DHS, DOD, and the State Department have additional budgets for pandemic preparedness for both domestic and international spending.
Although the 20th century experienced only 3 significant pandemics (the Spanish flu of 1918-19 and 2 influenza pandemics in 1957 and 1968) the mass media have presented us with almost non-stop pandemics during the 21st century: SARS-1 (2002-3), avian flu (2004-on), swine flu (2009-10), Ebola (2014, 2018-19), Zika (2016), COVID (2020-2023), and monkeypox (2022-23). And we are incessantly told that more are coming, and that they are likely to be worse.
We have been assaulted with warnings and threats for over 2 decades to induce a deep fear of infectious diseases. It seems to have worked.
The genomes of both SARS-CoV-2 and the 2022 monkeypox (MPOX) virus lead to suspicion that both were bioengineered pathogens originating in laboratories. The group of virologists assembled by Drs. Fauci and Farrar identified 6 unusual (probably lab-derived) parts of the SARS-CoV-2 genome as early as February 1, 2020 and more have been suggested subsequently.
I do not know if these viruses leaked accidentally or were deliberately released, but I am leaning toward the conclusion that both were deliberately released, based on the locations where they first appeared, the well-orchestrated but faked videos rolled out by the mass media for COVID, and the illogical and harmful official responses to each. In neither case was the public given accurate information about the infections’ severity or treatments, and the responses by Western governments never made scientific sense. Why wouldn’t you treat cases early, the way doctors treat everything else? It seemed that our governments were trading on the fact that few people knew enough about viruses and therapeutics to make independent assessments about the information they were being fed.
Yet by August 2021, there was no corresponding course correction. Instead, the federal government doubled down, imposing vaccine mandates on 100 million Americans in September 2021 in spite of ‘the science.’ There has been no accurate statement yet from any federal agency about the lack of utility of masking for an airborne virus (which is probably why the US government and WHO delayed acknowledging airborne spread by COVID for 18 months), the lack of efficacy of social distancing for an airborne virus, and the risks and poor efficacy of 2 dangerous oral drugs (paxlovid and molnupiravir) purchased by the US government for COVID treatment, even without a doctor’s prescription.
Never have any federal agencies acknowledged the truth about the COVID vaccines’ safety and efficacy. Instead, the CDC turns definitional and statistical cartwheels so it can continue to claim they are “safe and effective.” Even worse, with all that we know, a third generation COVID vaccine is to be rolled out for this fall and the FDA has announced that yearly boosters are planned.
All this goes on, even a year after we learned (with continuing corroborations) that children and working age adults are dying at rates 25 percent or more above the expected averages, and the vascular side effects of vaccination are the only reasonable explanation.
Maiming with Myocarditis
Both of the two US monkeypox/smallpox vaccines (Jynneos and ACAM2000) are known to cause myocarditis, as do all 3 COVID vaccines currently available in the US: the Pfizer and Moderna COVID-19 mRNA vaccines and the Novavax vaccine. The Novavax vaccine was first associated with myocarditis during its clinical trial, but this was downplayed and it was authorized and rolled out anyway, intended for those who refused the mRNA vaccines due to the use of fetal tissue in their manufacture.
Here is what the FDA’s reviewers wrote about the cardiac side effects noted in the Jynneos clinical trials:
Up to 18.4% of subjects in 2 studies developed post-vaccination elevation of troponin [a cardiac muscle enzyme signifying cardiac damage]. However, all of these troponin elevations were asymptomatic and without a clinically associated event or other sign of myopericarditis. p. 198
The applicant has committed to conduct an observational, post-marketing study as part of their routine PVP. The sponsor will collect data on cardiac events that occur and are assessed as a routine part of medical care. p. 200
In other words, while the only way to cause an elevated troponin level is to break down cardiac muscle cells, the FDA did not require a specific study to evaluate the extent of cardiac damage that might be caused by Jynneos when it issued its 2019 license. How frequently does myocarditis occur after these vaccines? If you use elevated cardiac enzymes as your marker, ACAM2000 caused this in one in thirty people receiving it for the first time. If you use other measures like abnormal cardiac MRI or echo, according to the CDC it occurs in one in 175 vaccinees. I have not seen a study with rates of myocarditis for Jynneos, but there was an unspecified elevation of cardiac enzymes in 10 percent and 18 percent of Jynneos recipients in two unpublished prelicensure studies available on the FDA website. My guess for the mRNA COVID vaccines is that they cause myocarditis in this general range, the vast majority of which remain undiagnosed and probably asymptomatic.
Why would our governments push 5 separate vaccines all known to cause myocarditis on young males who have been at extremely low risk from COVID, and who simply get a few pimples for 1-4 weeks from monkeypox unless they are immunocompromised? It’s an important question. It does not make medical sense. Especially when the vaccine probably does not work—Jynneos didn’t prevent infection in the monkeys in whom it was tested nor did it do well in people. And the CDC has failed to publish its trial of Jynneos vaccine in the ~1,600 Congolese healthcare workers on whom the CDC tested it for efficacy and safety in 2017. The CDC made the mistake of announcing the trial, and posting it to clinicaltrials.gov as required, but has not informed its advisory committee that reviewed the vaccine, nor the public, of the trial’s results.
There can be no question about it: our health agencies are guilty of malfeasance, misrepresentation, and deliberate infliction of harm on their own populations. The health agencies first incited terror with apocalyptic predictions, then demanded patients be medically neglected, and finally enforced vaccinations and treatments that were tantamount to malpractice.
COVID Vaccines: The Chicken or the Egg?
The health authorities could have just been ignorant—that could possibly explain the first few months of the COVID vaccines’ rollout. But once they figured out, and even announced in August 2021 that the vaccines did not prevent catching COVID or transmitting it, why did our health authorities still push COVID vaccines on low-risk populations who were clearly at greater risk from a vaccine side effect than from COVID? Particularly as time went on and newer variants were less and less virulent?
Once you acknowledge these basic facts, you realize that maybe the vaccines were not made for the pandemic, and instead the pandemic was made to roll out the vaccines. While we cannot be certain, we should at least be suspicious. And the fact that the US contracted for 10 doses per person (review purchases here, here, here, here and here) and so did the European Union (here and here) and Canada should make us even more suspicious–there is no justification for agreeing to purchase so many doses for vaccines at a time when the vaccines’ ability to prevent infection and transmission was questionable, and its safety suspect or worrying.
Why would governments want ten doses per person? Three maybe. But ten? Even if yearly boosters were expected, there was no reason to sign contracts for enough vaccine for the next nine years for a rapidly mutating virus. Australia bought 8 doses per person. By December 20, 2020 New Zealand had secured triple the vaccines it needed, and offered to share some with nearby nations. No one has come forward to explain the reason for these excessive purchases.
Furthermore, you don’t need a vaccine passport (aka digital ID, aka a phone app that in Europe included a mechanism for an electronic payments system) unless you are giving out regular boosters. Were the vaccines conceived of as the means for putting our vaccinations, health records, official documents–and most importantly, shifting our financial transactions online, all managed on a phone app? This would be an attack on privacy as well as the enabling step to a social credit system in the West. Interestingly, vaccine passports were already being planned for the European Union by 2018.
A Pandemic Treaty and Amendments: Brought to You by the Same People who Mismanaged the Past 3 Years, to Save us from Themselves?
The same US and other governments and the WHO that imposed draconian measures on citizens to force us to be vaccinated and take dangerous, expensive, experimental drugs, withheld effective treatments, and refused to tell us that most people who required ICU care for COVID were vitamin D-deficient and that taking vitamin D would lessen COVID’s severity–decided in 2021 we suddenly needed an international pandemic treaty. Why? To prevent and ameliorate future pandemics or biological warfare events… so we would not suffer again as we did with the COVID pandemic, they insisted. The WHO would manage it.
To paraphrase Ronald Reagan, the words, “I’m from the WHO, and I’m here to help” should be the most terrifying words in the English language after the COVID fiasco.
What the WHO and our governments conveniently failed to mention is that we suffered so badly because of their medical mismanagement and our governments’ merciless economic shutdowns and mismanagement. According to the World Bank, an additional 70 million people were forced into extreme poverty in 2020 alone. This was due to policies issued by our nations’ rulers, their elite advisers and the World Health Organization, which came out with guidance to shut down economic activity that most nations adopted without question. The WHO is acutely aware of the consequences of economic lockdowns, having published the following:
Malnutrition persisted in all its forms, with children paying a high price: in 2020, over 149 million under-fives are estimated to have been stunted, or too short for their age; more than 45 million – wasted, or too thin for their height…
Starvation may have killed more people than COVID, and they were disproportionately the youngest, rather than the oldest. Yet the WHO prattles on about equity, diversity, and solidarity—having itself caused the worst food crisis in our lifetime, which was not due to nature but was man-made.
How can anyone take seriously claims by the same officials who mishandled COVID that they want to spare us from another medical and economic disaster–by using the same strategies they applied to COVID, after they masterminded the last disaster? And the fact that no governments or health officials have admitted their errors should convince us never to let them manage anything ever again. Why would we let them draw up an international treaty and new amendments to the existing International Health Regulations (IHR) that will bind our governments to obey the WHO’s dictates forever?
Those dictates, by the way, include vaccine development at breakneck speed, the power to enforce which drugs we will be directed to use, and which drugs will be prohibited, and the requirement to monitor media for “misinformation” and impose censorship so that only the WHO’s public health narrative will be conveyed to the public.
The WHO’s Pandemic Treaty Draft Requires the Sharing of Potential Pandemic Pathogens. This is a Euphemism for Bioweapons Proliferation.
Obviously, the best way to spare us from another pandemic is to immediately stop funding gain-of-function (GOF) research and get rid of all existing GOF organisms. Let all nations build huge bonfires and burn up their evil creations at the same time, while allowing other nations to inspect their biological facilities and records.
But the WHO in its June 2023 Bureau Text of the Draft Pandemic Treaty has a plan that is the exact opposite of this. In the WHO’s draft treaty, which most nations’ rulers appear to have bought into, all governments will share all viruses and bacteria they come up with that are determined to have “pandemic potential” — share them with the WHO and other governments, putting their genomic sequences online. No, I am not making this up. (See screenshots from the draft treaty below.) Then the WHO and all the Fauci’s of the world would gain access to all the newly identified dangerous viruses. Would hackers also gain access to the sequences? This pandemic plan should make you feel anything but secure.
Fauci, Tedros, and their ilk at the WHO, and those managing biodefense and biomedical research for nation states are on one side, the side that gains access to ever more potential biological weapons, and the rest of us are on the other, at their mercy.
This poorly conceptualized plan used to be called proliferation of weapons of mass destruction—and it is almost certainly illegal. (For example, see Security Council resolution 1540 adopted in 2004.) But this is the plan of the WHO and of many of our leaders. Governments will all share the weapons.
The Genomic Sequencing Conundrum
And governments are to commit to building biolabs that must include genomic sequencing. No explanation has been forthcoming about why each nation needs to install its own genome sequencing laboratories. Of course, they would sequence the many viruses that will be detected as a result of the pathogen surveillance activities nations must perform, according to the WHO treaty draft. But the same techniques can be used to sequence human genomes. The fact that the EU, UK, and US are currently engaged in projects to sequence about 2 million of their citizens’ genomes provides a hint they may want to collect additional genomes of Africans, Asians, and others.
This might fly as simply sharing state-of-the-art science with our less-developed neighbors. But it is curious that there is so much emphasis on genomics, compared to an absence of discussion about developing repurposed drugs for pandemics in the draft treaty or IHR amendments.
But we can’t forget that virtually all developed nations, in lockstep, restricted the use of safe generic hydroxychloroquine, ivermectin, and related drugs during the pandemic. In retrospect, the only logical explanation for this unprecedented action was to preserve the market for expensive patentable drugs and vaccines, and possibly to prolong the pandemic.
Genomes offer great potential profits, as well as providing the substrate for transhumanist experiments that could include designer babies.
The latest version (aka the WHO Bureau draft) of the pandemic treaty can be accessed here. I provide screenshots to illustrate additional points.

Draft pages 10 and 11:




The WHO Treaty Draft Incentivizes Gain-of-Function Research
What else is in the Treaty? Gain-of-Function research (designed to make microorganisms more transmissible or more pathogenic) is explicitly incentivized by the treaty. The treaty demands that administrative hurdles to such research must be minimized, while unintended consequences (aka pandemics) should be prevented. But of course, when you perform this type of research, leaks and losses of agents can’t always be prevented. The joint CDC-USDA Federal Select Agent Program (FSAP) which keeps track of research on potential pandemic pathogens collects reports of about 200 accidents or escapes yearly from labs situated in the US. The FSAP annual report for 2021 notes:
“In 2021, FSAP received 8 reports of losses, 177 reports of releases, and no reports of thefts.”
Research on deadly pathogens cannot be performed without risks both to the researchers and the outside world.
Draft page 14:

Vaccines Will be Rolled Out Speedily Under Abbreviated Future Testing Protocols
Vaccines normally take 10-15 years to be developed. In case you thought the COVID vaccines took too long to be rolled out (326 days from availability of the viral sequence to authorization of the first US COVID vaccine) the WHO treaty draft has plans to shorten testing. There will be new clinical trial platforms. Nations must increase clinical trial capacity. (Might that mean mandating people to be human subjects in out-of-the-way places like Africa, for example?) And there will be new “mechanisms to facilitate the rapid interpretation of data from clinical trials” as well as “strategies for managing liability risks.”
Draft page 14:


Manufacturer and Government Liability for Vaccine Injuries Must be “Managed”
Nations are supposed to use “existing relevant models” as a reference for compensation of injuries due to pandemic vaccines. Of course, most countries do not have vaccine injury compensation schemes, and when they do the benefits are usually minimal.
Is the US government’s program to be a model of what gets implemented internationally?
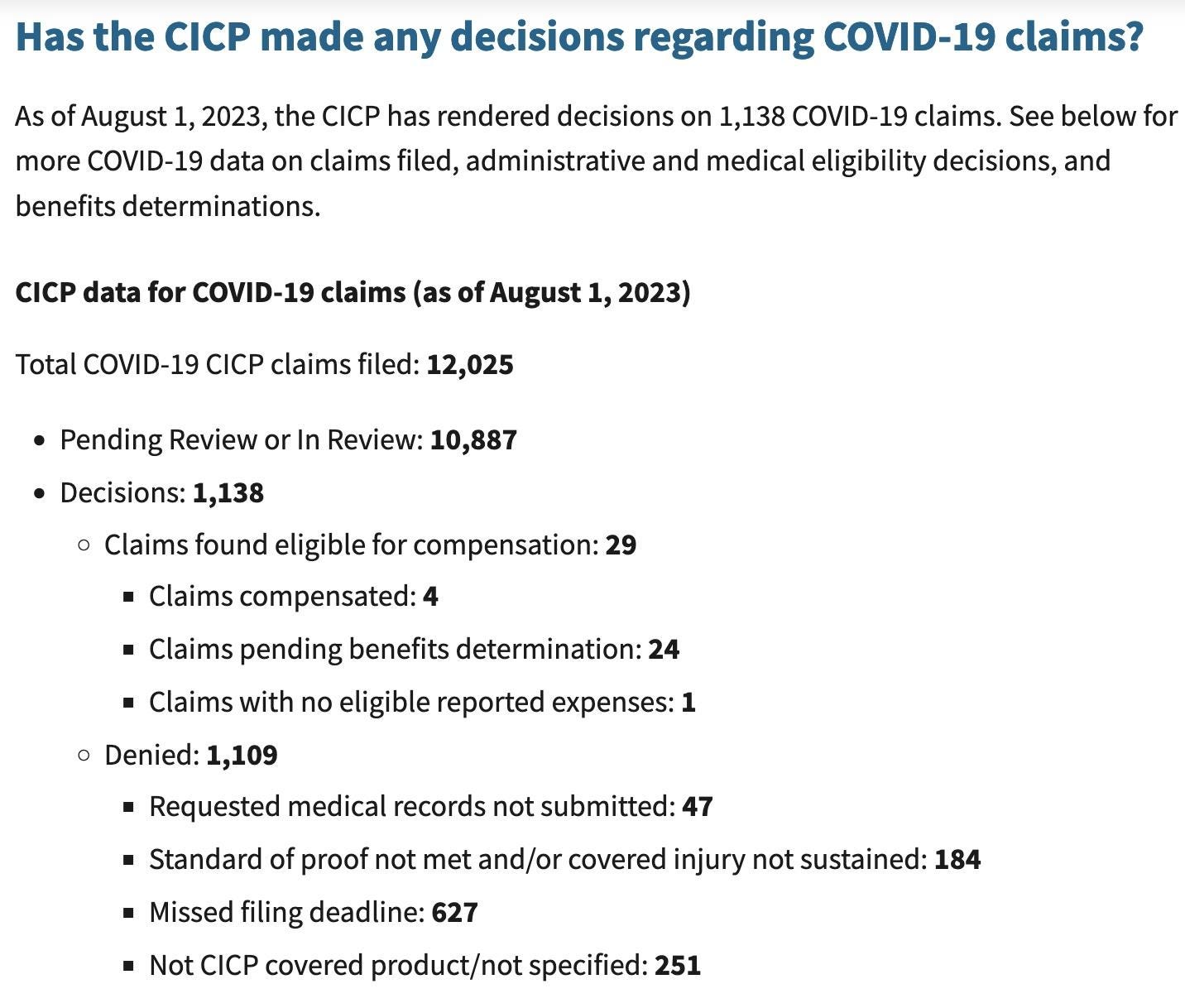
The US government scheme for injuries due to COVID pandemic products (the Countermeasures Injury Compensation Program or CICP) has compensated exactly 4 (yes, four) of the 12,000 claimants for COVID product-related injuries as of August 1, 2023. All pandemic EUA drugs and vaccines convey a liability shield to the government and manufacturers (this includes monoclonal antibodies, pre-licensure remdesivir, paxlovid, molnupiravir, some ventilators and all COVID vaccines) and the only avenue for injury compensation is through this program.
Slightly over 1,000 of the 12,000 claims have been adjudicated while 10,887 are pending review. Twenty claims were deemed eligible and await a benefits review. Benefits are only paid for uncovered medical expenses or lost income. A total of 983 people, or 98 percent of those whose claims have been adjudicated had their claims denied, many because they missed the brief one-year statute of limitations. Below are the latest data from this program:
The treaty draft also demands weakening the strict regulation of medical drugs and vaccines during emergencies, under the rubric of “Regulatory Strengthening.” As announced in the UK last week, where ‘trusted partner’ approvals will be used to speed licensure, this is moving toward a single regulatory agency approval or authorization, to be immediately adopted by other nations (p 25).

Next Up: Vaccines Developed in 100 Days
A plan to develop vaccines in 100 days and have them manufactured in 30 additional days has been widely publicized by the vaccine nonprofit CEPI, founded in 2017 by Sir Dr. Jeremy Farrar, who is now the WHO’s Chief Scientist. The plan has been echoed by the US and UK governments and received some buy-in from the G7 in 2021. This timeframe would only allow for very brief testing in humans, or would, more likely, limit testing to animals. Why would any country sign up for this? Is this what we the people want?
The plan furthermore depends on the vaccines only being tested for their ability to induce antibodies, which is termed immunogenicity, rather than being shown to actually prevent disease, at least for the initial rollout. My understanding of FDA regulation was that antibody levels were not an acceptable surrogate for immunity unless they had been demonstrated to actually correlate with protection. However, the FDA’s recent vaccine decisions have scrapped all that and vaccines are now being approved based on antibody titers alone. The FDA’s vaccine advisory committee has asked it for better indicators of efficacy than this, but the advisers have also voted to approve or authorize vaccines in the absence of any real measures showing that they work. I learned this because I watch the FDA vaccine advisory meetings and provide a live blog of them.
We all know how long it took for the public to become aware that the COVID vaccines failed to prevent transmission and only prevented cases for a period of weeks to months. The US government has still not officially admitted this, even though CDC Director Rochelle Walensky told CNN’s Wolf Blitzer the truth about transmission on August 6, 2021.
It is critical for the public to understand that safety testing can only be accomplished in human beings, as animals react differently to drugs and vaccines than humans do. Therefore, limited testing in animals would mean there was no actual safety testing. But testing vaccines in humans for only short periods is also unacceptable.
Testing vaccines during brief trials in humans (the Pfizer trials only followed a “safety subset” of trial subjects for a median of two months for safety) allowed COVID vaccines to be rolled out without the public being aware they could cause myocarditis and sudden deaths, most commonly in athletic young males in their teens and twenties, or a myriad of other conditions.
Finally, following this rapid manufacturing plan, thorough testing for potential failures in the manufacturing process could not be performed. With the current plan for far-flung, decentralized manufacturing facilities that are said to be necessary to achieve vaccine equity for all, there are nowhere near enough regulators who could inspect and approve them.
Will the WHO Respect Human Rights?
The need to respect “human rights, dignity, and freedom of persons” is embedded in the current International Health Regulations (IHR), as well as other UN treaties. However, the language guaranteeing human rights, dignity, and freedom of persons was peremptorily removed from the proposed IHR Amendments, without explanation. The removal of human rights protections did not go unnoticed, and the WHO has been widely criticized for it.
The WHO apparently is responding to these criticisms, and so the language guaranteeing human rights that was removed from the drafts of the International Health Regulations has been inserted into the newest version of the pandemic treaty.
Conclusions
As long predicted by science fiction, our bio- and cyber-scientific achievements have finally gotten away from us. We can produce vaccines in 100 days and manufacture them in 130 days–but there will be no guarantees that the products will be safe, effective, or adequately manufactured. And we can expect large profits but no consequences for the manufacturers.
Our genes can be decoded, and the fruits of personalized medicine made available to us. Or perhaps our genes will be patented and sold to the highest bidder. We might be able to select for special characteristics in our children, but at the same time, a human underclass could be created.
Our electronic communications can be completely monitored and censored, and uniform messaging can be imposed on everyone. But for whom would this be good?
New biological weapons can be engineered. They can be shared. Maybe that will speed up the development of vaccines and therapeutics. But who really benefits from this scheme? Who pays the price of accidents or deliberate use? Wouldn’t it be better to end so-called gain-of-function research entirely through restrictions on funding and other regulations, rather than encouraging its proliferation?
These are important issues for humanity, and I encourage everyone to become part of the conversation.
Dr Nass. Of course your website stopped working. You are a clear and present danger to the power brokers. Thank you for your incredible energy to keep it up.
Your erudite, well researched and accurate article covers the bases.
I suspect the attention span of influencers outside our rapidly inflating bubble have an attention span of around 5 minutes at most.
Might I suggest an executive summary of sorts?
Bullet points might be:
The US has engaged in biological warfare for decades and has a massive budget to continue doing so.
Examples - maybe from RFK jr's book "The Real..Voldemoort(s)" on how federal agencies experimented on deprived kids in the US - and thousands of women in Africa and India
The powers given to HHS secretaries is a breach of the Constitution
The powers given to the WHO are also a breach - Sovereignty cannot be delegated to a third party.
The WHO has insufficient competence to handle the task it is seeking to control - national health systems are struggling - the WHO would make things far worse as it has no track record or competence (who the hell hires WHO staff on what basis???)
You are a good person - trouble is the Cult is not. I would get someone to frame the issues you raise in a brutal way in those bullet points. We are at war after all.