


Negative COVID vaccine efficacy. When the remedy becomes the poison
These vaccines poison in multiple ways, but here I am confining the evidence to the vaccine-caused increase in susceptibility to the infection it was intended to prevent

This is a CDC slide. The data are from CDC’s ICATT study. I screen shot it at an ACIP meeting a couple of years ago. I think there are some issues with it, but the consistency of the data, despite different age groups, cannot be ignored.
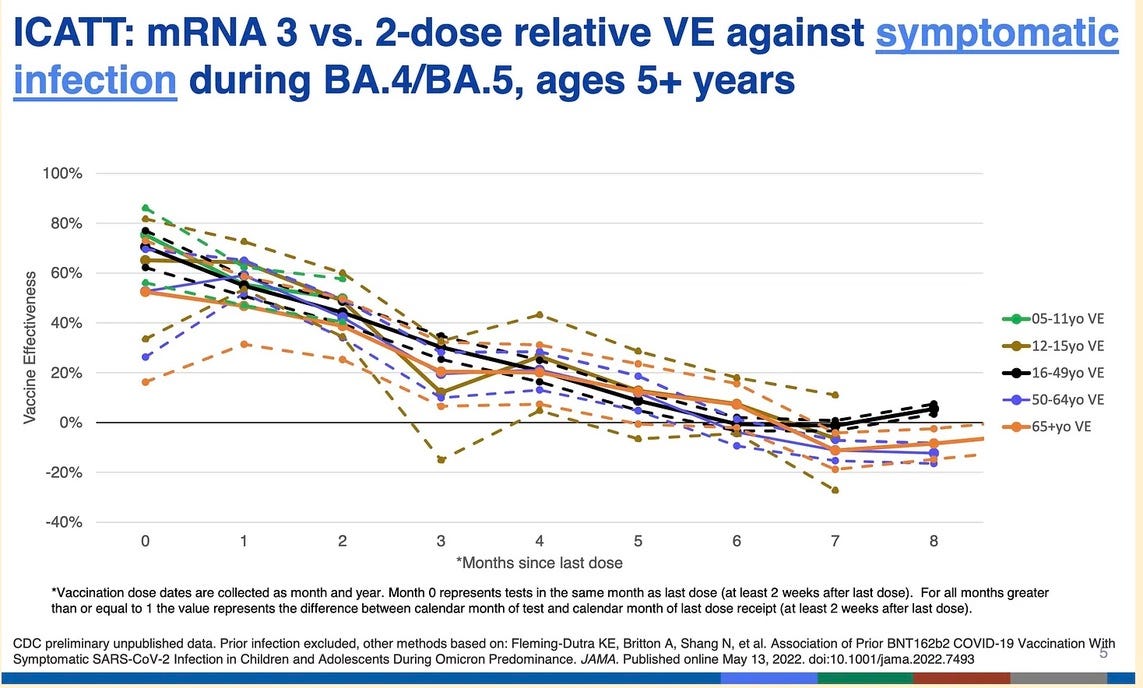
At about 6-7 monthsfor all age groups, whether you received 2 or 3 shots in total, effectiveness drops to zero. Then they stop collecting data, but it looks like efficacy is negative after that.
The JAMA published data on all children in NY state regarding vaccine efficacy. The state knew the date of every shot for every child, and the date of every COVID test.
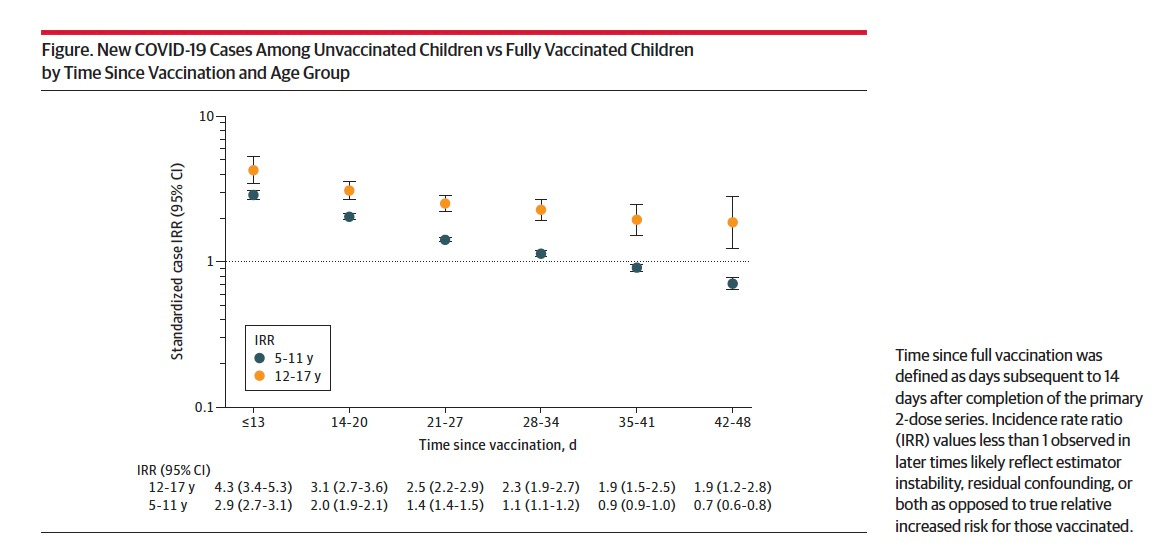
In this graph, the time since the child was designated “fully vaccinated”—2 weeks after the second shot—is measured in days, not months, along the X axis.
The orange dots are children 12-17 years old, who received an adult dose but on average weigh half what an adult weighs.
The black dots are children aged 5-11 years old, who received 1/3 the adult dose if they got Pfizer, and approximately that much less for the other vaccines.
The horizontal lines associated with the dots indicate that the reliability of the data is extremely robust, as this involved information from several million children and it is consistent.
By six weeks after being “fully immunized” the younger children have already reached negative efficacy, and they continue to drop at week 7, when the data collection is cut off. These important data were buried in a JAMA letter (although featured in the NY Times in an article by Apoorva Mandavilli) and the text of the letter did not explain them.
I have written about both these graphs previously. I also wrote about Israeli data that showed increased susceptibility to infection over about two weeks post-second shot.
Professor Raphael Lataster has just managed to get his analysis of negative COVID vaccine efficacy into a top journal in Australia. Yet again, as a letter. It seems the censorship of letters is a bit less than the censorship of articles. So here is Raphael’s analysis:
https://www1.racgp.org.au/ajgp/2024/july/letters
For example, a recent The Lancet Regional Health paper states: ‘Compared to a waned third dose, fourth dose VE [vaccine effectiveness] was 13.1% (95% CI 0.9 to 23.8) overall; 24.0% (95% CI 8.5 to 36.8) in the first two months post-vaccination, reducing to 10.3% (95% CI −11.4 to 27.8) and 1.7% (95% CI −17.0 to 17.4) at two to four and four to six months, respectively’.2 Given the wide confidence intervals, these latter figures could be negative. A study by Shrestha et al found each vaccine dose was associated with a higher number of infections, with those on zero doses faring best.3 A study published in the New England Journal of Medicine found vaccine effectiveness dropping dramatically, including for severe COVID, with the previously infected and unvaccinated having lower infection rates than the never-infected double dosed.4 And a British study revealed the effectiveness of one to two doses of AstraZeneca and Pfizer vaccines dropping to zero, and turning negative, after only two to three months.5 There is much more in the literature; word count prevents me from listing all such evidence.
Relatively few articles dare to explicitly discuss the phenomenon of perceived COVID-19 vaccine negative effectiveness, though Monge et al at least acknowledged it and tried to explain it away with a hypothesis around some selection bias.6 A British Medical Journal (BMJ) rapid response listed some of the evidence for this disturbing phenomenon, and called for further research.7 Furthermore, an unofficial ‘series’ of four articles, involving Peter Doshi, in the Journal of Evaluation in Clinical Practice, the last of which was published this year, indicates that issues with counting windows have likely led to exaggerations of COVID-19 vaccine effectiveness and safety estimates, for both the clinical trials and later observational studies.8 Finally, in contrast to Monge et al, a new Czech study by Fürst et al found strong evidence for the healthy vaccinee effect;9 this also seems to be evident in the recent and much-publicised Australian study promoting booster shots, which revealed an uncharacteristically high unvaccinated rate in elderly Australian aged care residents.10
All this makes it plausible that the COVID-19 vaccines have always had an effectiveness that was very low, zero, or even negative, with inadequate methods allowing for a highly exaggerated effectiveness initially – an exaggeration that is lessened with time. It is, as Professor Tindle noted, possible that the vaccines could be causing immunosuppression. With the ubiquitousness of the vaccines, and the fact that some vaccine mandates are still in place, to say nothing of the upcoming Senate inquiry into excess mortality,11 I suggest we investigate this further.
Author
Raphael Lataster BPharm, PhD, Associate Lecturer, FASS, University of Sydney, Sydney, NSW
Competing interests: None.
References
Tindle R. Long COVID: Sufferers can take heart. Aust J Gen Pract 2024;53(4):238–40. doi: 10.31128/AJGP-07-23-6896.
Kirwan PD, Hall VJ, Foulkes S, et al; SIREN Study Group. Effect of second booster vaccinations and prior infection against SARS-CoV-2 in the UK SIREN healthcare worker cohort. Lancet Reg Health Eur 2023;36:100809. doi: 10.1016/j.lanepe.2023.100809.
Shrestha NK, Burke PC, Nowacki AS, Simon JF, Hagen A, Gordon SM. Effectiveness of the coronavirus disease 2019 bivalent vaccine. Open Forum Infect Dis 2023;10(6):ofad209. doi: 10.1093/ofid/ofad209.
Goldberg Y, Mandel M, Bar-On YM, et al. Protection and waning of natural and hybrid immunity to SARS-CoV-2. N Engl J Med 2022;386(23):2201–12. doi: 10.1056/NEJMoa2118946.
Kerr S, Bedston S, Bradley DT, et al. Waning of first- and second-dose ChAdOx1 and BNT162b2 COVID-19 vaccinations: A pooled target trial study of 12.9 million individuals in England, Northern Ireland, Scotland and Wales. Int J Epidemiol 2023;52(1):22–31. doi: 10.1093/ije/dyac199.
Monge S, Pastor-Barriuso R, Hernán MA. The imprinting effect of covid-19 vaccines: An expected selection bias in observational studies. BMJ 2023;381:e074404. doi: 10.1136/bmj-2022-074404.
Lataster R. We need proper explanations for apparent COVID-19 vaccine negative effectiveness. BMJ 2023;381. Available at www.bmj.com/content/381/bmj-2022-074404/rr-0 [Accessed 24 May 2025].
Lataster R. How the adverse effect counting window affected vaccine safety calculations in randomised trials of COVID-19 vaccines. J Eval Clin Pract 2024;30(3):453–58. doi: 10.1111/jep.13962.
Fürst T, Bazalová A, Fryčák T, Janošek J. Does the healthy vaccinee bias rule them all? Association of COVID-19 vaccination status and all-cause mortality from an analysis of data from 2.2 million individual health records. Int J Infect Dis 2024;142:106976. doi: 10.1016/j.ijid.2024.02.019.
Lin L, Demirhan H, P Johnstone-Robertson S, Lal R, M Trauer J, Stone L. Assessing the impact of Australia’s mass vaccination campaigns over the Delta and Omicron outbreaks. PLoS One 2024;19(4):e0299844. doi: 10.1371/journal.pone.0299844.
Parliament of Australia. Excess mortality. Parliament of Australia, 2024. Available at www.aph.gov.au/Parliamentary_Business/Committees/Senate/Community_Affairs/ExcessMortality47 [Accessed 24 May 2024].
“fully vaccinated”—2 weeks after the second shot
Don't forget Professors Fenton and Neil have already shown at wherearethenumbers.substack.com that using such a delay in vaccination status completely invalidates the official efficacy.
Calling an experimental, unproven, toxic snake oil a "Vaccine" from our 60 Billion in fraud fines and leader in cause of iatrogenic/ [medicine caused] death, is the same type of fraud big pharma uses on chumps and suckers, "Born every minute." So just Stop it!!! Call it what it is, not what shysters identify it as!