


What are FDA's criteria for issuing a COVID vaccine EUA? What happens when Pfizer and Moderna vaccines fall short? Next up, babies and toddlers

FDA made it very clear what its standards were for COVID vaccines.
FDA repeatedly told its advisory committee, the public and vaccine manufacturers what it required in order to issue an EUA for a COVID vaccine. I have copied 4 of the FDA's power-points below so we can all agree on what, precisely, those standards are.
Then we can all agree on something else. Those standards turned out to look like a high-jumper's bar. The vaccine, like the high-jumper, only has to get up over the bar for a brief moment in time. That moment occurred exactly 2 months and 2 weeks after getting a second mRNA shot. Earlier than that, the vaccine couldn't reach the bar. After that brief moment, vaccine efficacy, like the high-jumper, came crashing down.

The slides below come from a presentation that was given before the FDA's Vaccine and Related Biologic Products Advisory Committee (VRBPAC) on December 10, 2020, when the committee was considering giving Pfizer's vaccine an Emergency Use Authorization. The slides echoed what had been said at earlier meetings of the VRBPAC and the guidance for industry FDA had published.
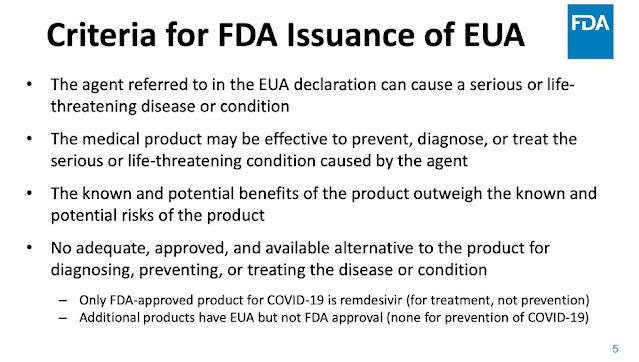
Notice the loose terminology: the medical product "may" be effective. Not exactly what you were expecting from the FDA, right? But this is the statutory standard built into all EUA products. When Congress passed the statute they thought they were shielding us against some brief emergency, it would be okay just to hope a medical product worked. After all, the FDA is here to protect the public health, right? They would never give us a bad product. They would never withhold the safety and efficacy data now, would they?
The statute simply says that to issue an EUA, the known and potential risks are outweighed by the known and potential benefits. Not a high bar. That pesky term "potential" is a loophole you could drive a truck through. Looked at another way, the vaccine is only expected to kill less people than it saves.
Is that the standard you want for injecting the entire country (or world) with an entirely novel bit of technology, which includes mRNA and two different lipids (3 separate molecules) never before injected into humans?
The last criterion on the second slide (#5) says there must be no adequate, approved (i.e., licensed) available alternative in order to issue an EUA for an experimental product. That is exactly the language in the statute, and FDA echoes it in many of its presentations and documents.
For those who have not yet heard me rant on this subject, this is precisely why FDA and the other federal agencies can NEVER, no matter how much evidence accrues, admit that hydroxychloroquine, ivermectin or any other licensed drug can treat and/or prevent COVIID--because if they admitted it, they will have admitted that they illegally issued EUAs to other drugs, vaccines, monoclonal antibodies, convalescent serum, etc.
The third slide (#6) says manufacturing should be of good quality and product should be uniform. We know that under the best of circumstances, the intact mRNA at the factory varied form about 50% to 75% and the so-called degradation products or visible particulates were not characterized. The important thing is what is in the product after it has withstood multiple episodes of shipping. (The components are made in different places and bottling may occur in a third place.) I don't know if such studies were performed. I doubt FDA did inspections on-site during 2020 in Germany and other countries where components were made, because elsewhere I read FDA did no international inspections that year.
(#6) also says there should be extensive ("clear and compelling") safety and efficacy data, sufficient to using the product in hundreds of millions of people. And that the collection of these data should be ongoing.
The final slide, (#7) is quite interesting. It specifies that efficacy should be at least 50%. Furthermore, FDA wants to study cases of severe disease. It says there need to be enough of them, especially because severe disease can also indicate antibody-enhanced disease aka vaccine-enhanced disease (VED).
In other words, FDA was concerned about the possibility that being vaccinated might lead to a worse COVID outcome, as had happened in animal studies of older coronavirus vaccine prototypes, and in an RSV vaccine trial in infants, and in a very early, licensed measles vaccine around 1960. And in the Dengue vaccine (Sanofi's Dengvaxia) in some Philippino children, where dozens died. Sanofi employees and health officials in Philippines stood trial for manslaughter over that debacle.
What did FDA do? FDA quietly licensed the identical vaccine in the US for kids aged 9 through 16, if they have evidence of a prior Dengue infection, which is thought to prevent VED. CDC recommended it.
Back to COVID vaccines. So to issue an EUA, FDA wanted severe COVID cases in the vaccinated to be evaluated, to be sure there was no VED occurring, in other words, to be assured the vaccine was not making their COVID worse.
Fast forward from December 2020 to April 2022. FDA is about to consider issuing an EUA for Moderna and Pfizer vaccines in the 6 month up to 5 year age group. But there were no serious cases of COVID in Moderna's clinical trial, and supposedly there were no severe cases in earlier Pfizer trials of older children.
Therefore, the standard FDA laid out in 2020 can't be met.
There is also no 50% efficacy. Moderna claimed its vaccine was 40% efficacious in the littlest kids (they claimed 94.5% for adults). CDC claimed Pfizer's vaccine was 31% effective in 5-11 year olds at about 7 weeks, and the NY Department of Health said Pfizer's vaccine had dropped to 12% efficacy in about 7 weeks.
So what's a poor FDA to do?
Only we can stop them from issuing that EUA.


"Only we can stop them from issuing that EUA" Please, tell us how to go about doing this...it seems we are running out of time..... :(
Meryl, it seems the 50% is not only just a guidance, it is also an arbitrary level. So I think they can easily change it to approve a vaccine. There is no science to the 50%. The person who came up with that likely had 5 fingers/hand. If they had a finger missing, the guidance would have been 40% ...